Our finest software engineers worked hard to obtain the PDF editor we are delighted to present to you. This application allows you to effortlessly create how do you request a cash out for modern woodman and saves precious time. You need to simply follow this guideline.
Step 1: Choose the button "Get Form Here".
Step 2: Now you can change your how do you request a cash out for modern woodman. Our multifunctional toolbar enables you to include, delete, change, and highlight text as well as carry out other commands.
Type in the data demanded by the platform to prepare the file.
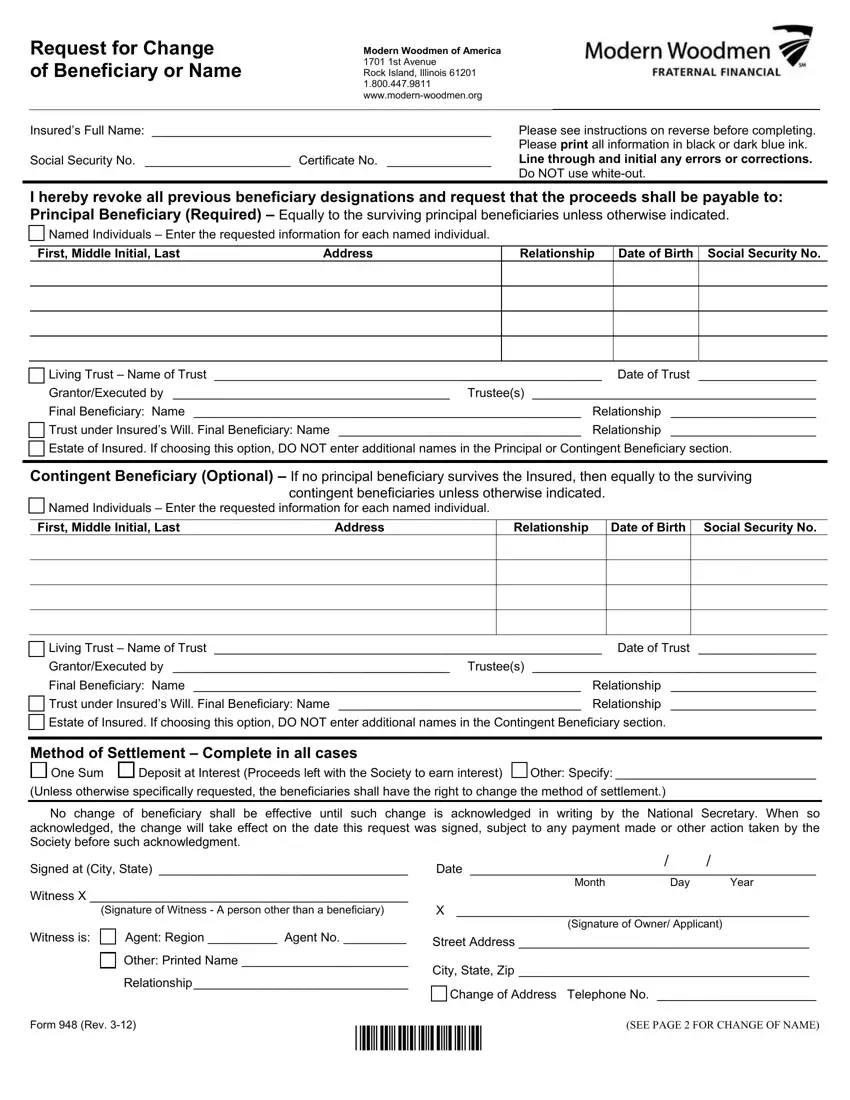
In the segment Contingent Beneficiary Optional, Named Individuals Enter the, contingent beneficiaries unless, First Middle Initial Last, Address, Relationship, Date of Birth, Social Security No, Living Trust Name of Trust Date, Estate of Insured If choosing this, Method of Settlement Complete in, No change of beneficiary shall be, Signed at City State, Witness X, and Date provide the particulars which the program requests you to do.
You may be required some fundamental information so you can prepare the Signature of Witness A person, Signature of Owner Applicant, Witness is Agent Region Agent No, Street Address, Other Printed Name, Relationship, City State Zip, Change of Address Telephone No, Form Rev, and SEE PAGE FOR CHANGE OF NAME box.
Please record the rights and responsibilities of the sides inside the Request for Name Change Insureds, Insured, Certificate Number, The name of the Owner has been, New complete legal name First, The reason for the change is, If selecting Other please provide, X Date, Signature of Insured or Owner, Month, Day, Year, X Signature of Witness, Witness is Agent Region Agent No, and Instructions for Change of paragraph.
Step 3: Select the Done button to save your document. Then it is obtainable for transfer to your device.
Step 4: Generate copies of your form. This may protect you from potential future misunderstandings. We do not look at or reveal your data, for that reason be certain it will be secure.
