The PDF editor will make completing files trouble-free. It is quite straightforward to update the [FORMNAME] form. Use the following steps if you want to do it:
Step 1: Select the button "Get Form Here" and select it.
Step 2: You can see all the functions which you can take on your template once you have entered the m t bank beneficiary claim form editing page.
You should type in the next details to create the m t bank beneficiary claim form PDF:
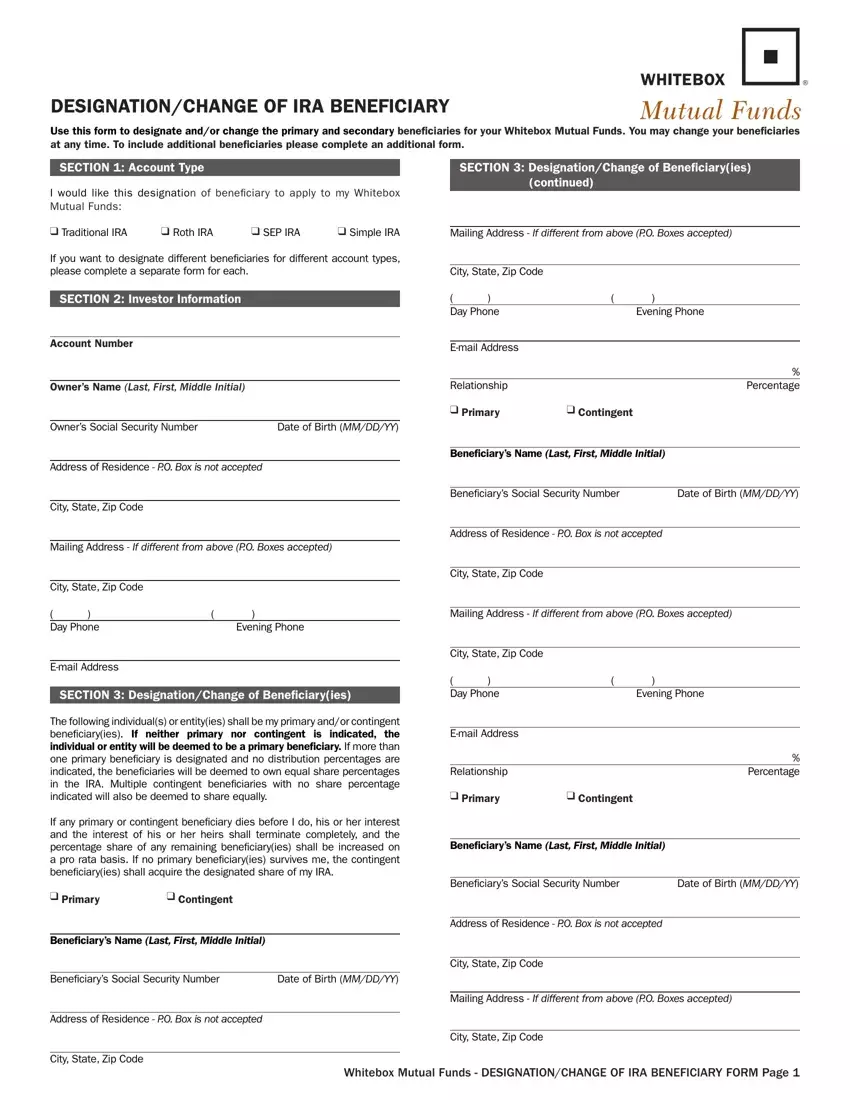
Provide the required details in the area Day Phone Evening Phone, Email Address, SECTION DesignationChange of, The following individuals or, If any primary or contingent, q Primary, q Contingent, Beneiciarys Name Last First Middle, Beneiciarys Social Security Number, Date of Birth MMDDYY, Address of Residence PO Box is, City State Zip Code, Mailing Address If different from, City State Zip Code, and Day Phone Evening Phone.
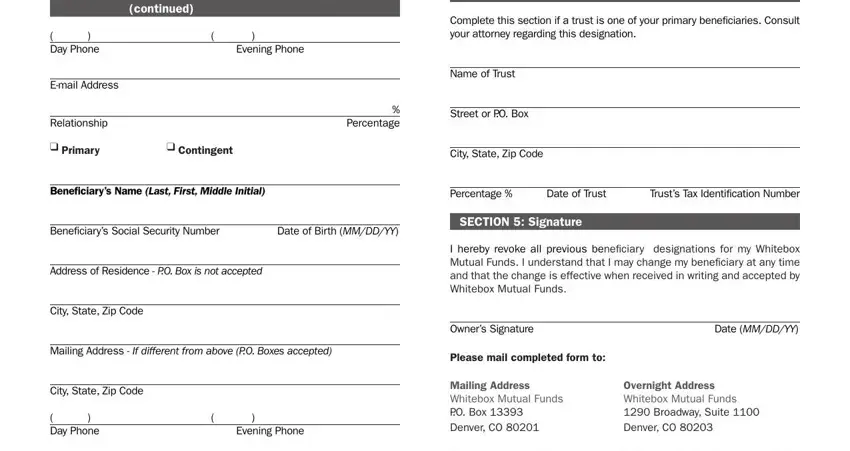
Indicate the necessary details in SECTION DesignationChange of, SECTION Trust Beneiciaryies, continued, Day Phone Evening Phone, Complete this section if a trust, Email Address, Relationship, q Primary, Name of Trust, Percentage, Street or PO Box, q Contingent, City State Zip Code, Beneiciarys Name Last First Middle, and Percentage Date of Trust field.
Inside the paragraph If you have any questions please, Email Address, Relationship, Percentage, Spousal Consent This section, CURRENT MARITAL STATUS, q I Am Not Married I understand, q I Am Married I understand that, CONSENT OF SPOUSE I am the spouse, and I hereby give the IRA holder any, identify the rights and obligations of the parties.
Step 3: As soon as you click on the Done button, the final file is easily transferable to all of your devices. Alternatively, you may send it by means of email.
Step 4: Make sure to stay clear of potential misunderstandings by creating at least a couple of duplicates of the document.
