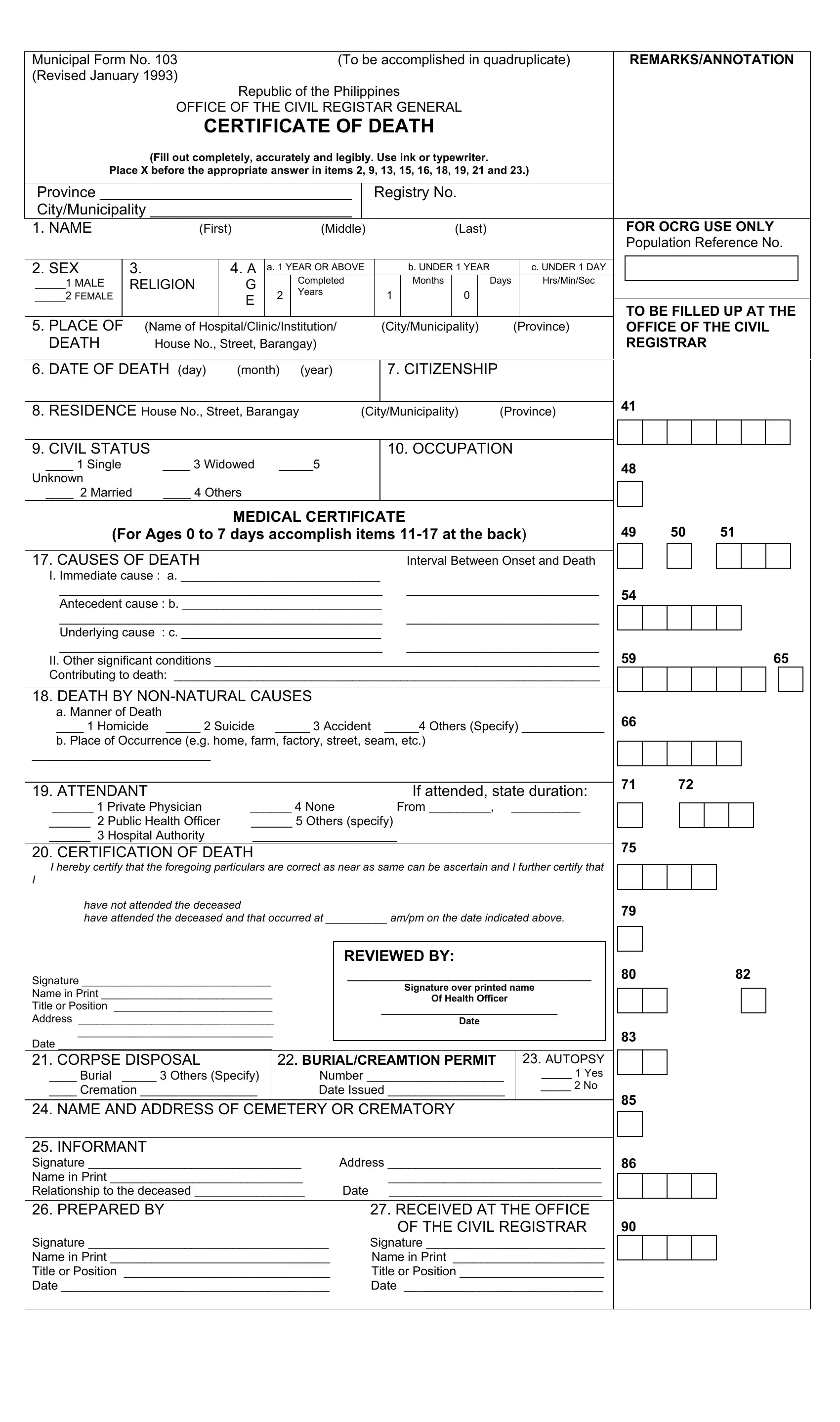
Navigating the intricacies of dealing with a loved one's passing involves several bureaucratic steps, one of which is completing the Municipal Form No. 103. Required to be filled out in quadruplicate and revised as of January 1993, this form serves as a pivotal document within the Republic of the Philippines for officially recording deaths. It demands a meticulous level of detail concerning the deceased, including basic identification, the circumstances of death, and specific choices regarding the disposition of the body. Enumerated sections require information on the deceased's sex, age, citizenship, civil status, and medical causes of death, alongside indications for autopsy and burial or cremation preferences. Additionally, the form addresses whether the death resulted from natural or non-natural causes and includes a separate medical certificate for infants who pass away between 0 to 7 days old. Certifications by health officials and embalmers are also integral parts of the form, ensuring that all facts surrounding the death are accurately and officially recorded. The document is further comprised of affidavits for delayed registrations, making the Municipal Form No. 103 a comprehensive record that facilitates the legal and procedural acknowledgment of death within the jurisdiction of the Philippine civil registry system.
| Question | Answer |
|---|---|
| Form Name | Municipal Form No 103 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | death certificate form philippines, sample death certificate philippines, death certificate form download, sample of death certificate in philippines |