
253g 2 can be completed effortlessly. Just use FormsPal PDF editor to perform the job promptly. Our tool is continually developing to provide the best user experience attainable, and that is due to our commitment to continual enhancement and listening closely to user comments. If you're looking to start, this is what it will require:
Step 1: Simply hit the "Get Form Button" at the top of this page to get into our form editing tool. Here you'll find everything that is required to work with your document.
Step 2: With the help of this online PDF tool, you are able to accomplish more than simply fill in blank form fields. Edit away and make your forms appear high-quality with customized text added in, or optimize the original content to perfection - all comes along with an ability to incorporate any images and sign it off.
Be attentive when filling in this pdf. Make sure all required blank fields are completed properly.
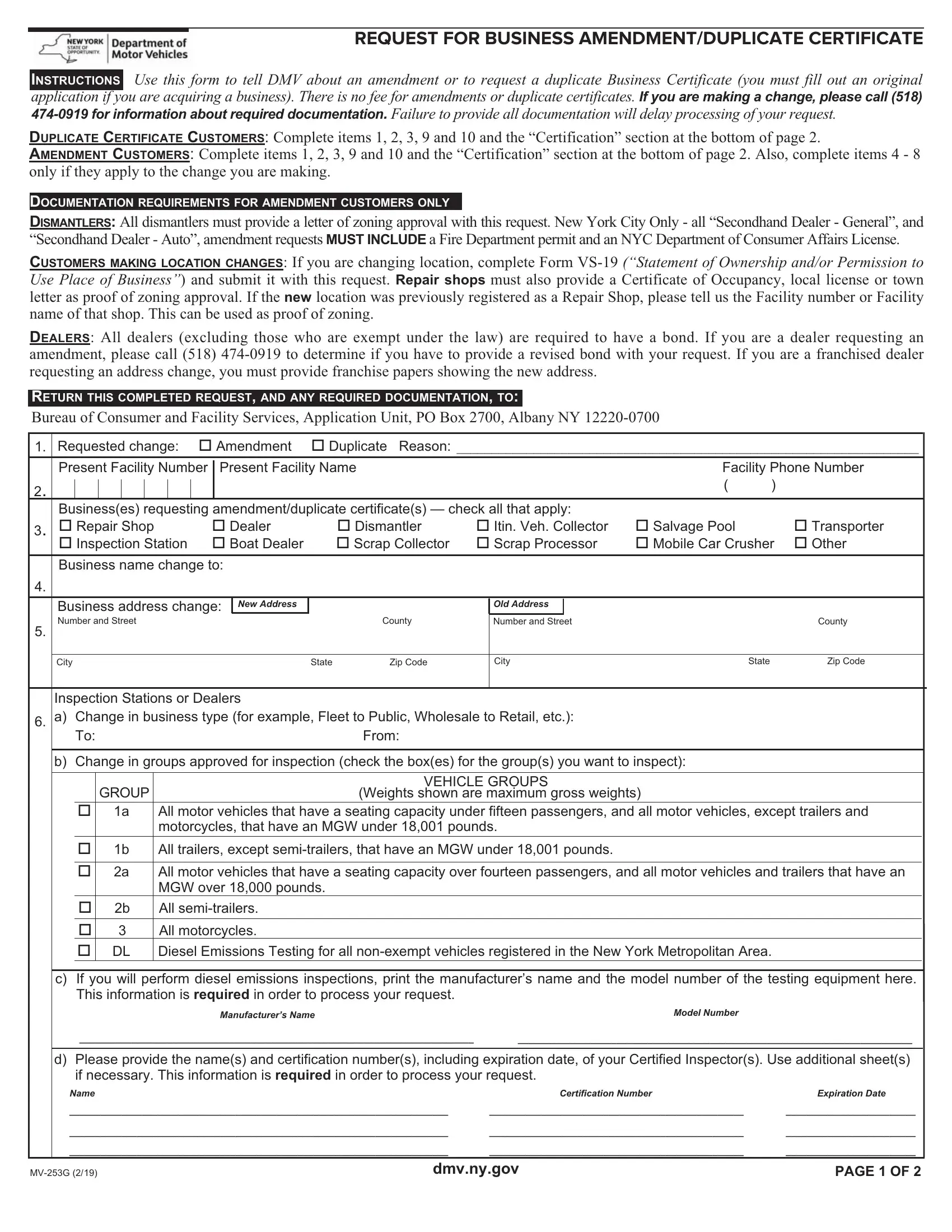
1. To start off, while filling in the 253g 2, begin with the section that has the next fields:
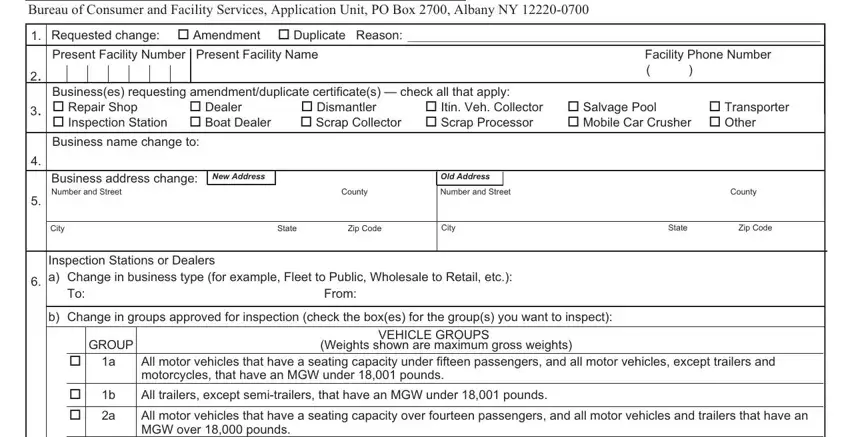
2. After this section is finished, you're ready to put in the required details in a All motor vehicles that have a, c If you will perform diesel, Manufacturers Name, Model Number, d Please provide the names and, Name, Certification Number, Expiration Date, MVG, dmvnygov, and PAGE OF so that you can move on further.
3. In this particular stage, look at Deletions to Owners Partners, Present Facility Number Present, a Name First MI Last, Please Sign Name in Full, X Residence Address, b Name First MI Last, Please Sign Name in Full X, c Name First MI Last, Please Sign Name in Full, X Residence Address, Date of Birth, Title, of Stock or Ownership, Driver License Identification, and Social Security Number. Each of these must be filled in with highest precision.
4. To move ahead, this fourth step involves filling in a few blanks. These include X Residence Address, c Name First MI Last, Please Sign Name in Full, X Residence Address, Apt No, Residence Phone, Date of Birth, Title, of Stock or Ownership, Driver License Identification, Social Security Number, Apt No, Residence Phone, a Have you or has any person named, and b Are you or is anyone named in, which are essential to continuing with this particular PDF.
When it comes to X Residence Address and Title, make sure that you double-check them in this current part. Both these are thought to be the most important fields in the document.
5. As you come near to the finalization of the file, there are a few extra points to undertake. In particular, NOTE For partnerships each partner, Name Please Print Full Name, Signature Full Name X, Partners Signature Full Name, MVG, Title, Partners Signature Full Name, Business Phone Number, Date, resetclear, and PAGE OF must all be filled out.
Step 3: Right after taking one more look at your fields and details, hit "Done" and you are all set! Create a free trial subscription with us and acquire direct access to 253g 2 - with all transformations saved and accessible in your personal account page. At FormsPal.com, we endeavor to guarantee that all your details are stored private.