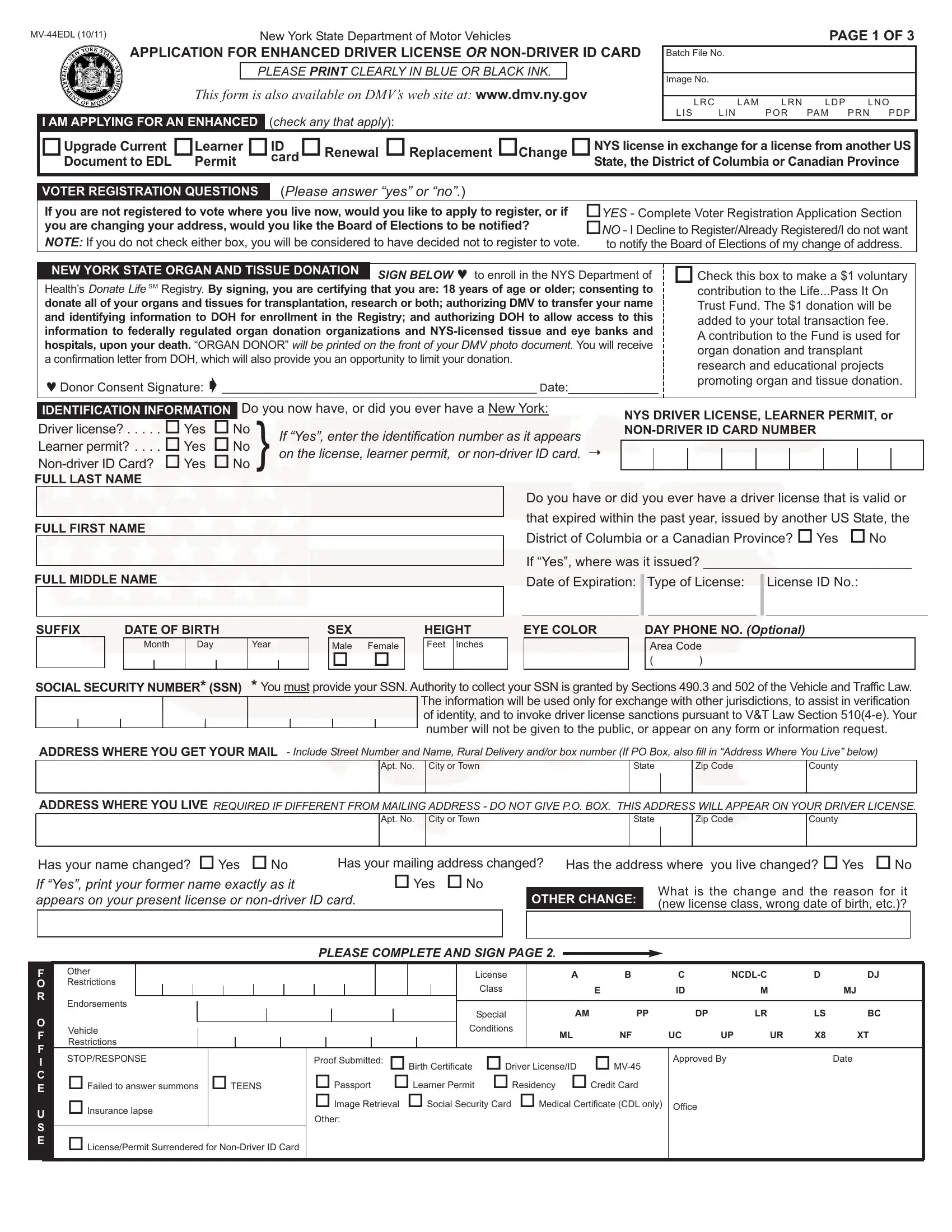
In the landscape of documentation required for driving and identification purposes in the United States, particularly in New York State, the MV-44EDL form serves as a pivotal document for individuals seeking an Enhanced Driver License (EDL) or Non-Driver ID Card. This form, set forth by the New York State Department of Motor Vehicles, encompasses various critical elements extending beyond mere application for a new, renewed, or replacement document. It integrally ties the user's application process to broader civic responsibilities and utilities, such as voter registration and organ donation consent, thereby embedding a layer of social responsibility within a routine administrative procedure. Applicants are prompted to provide detailed personal identification information, and have the option to address changes in their information, thereby ensuring the state's records remain accurate and up-to-date. Additionally, through the MV-44EDL, the offer to contribute to the Life..Pass It On Trust Fund directly from the form facilitates easy participation in broader community support activities, such as organ donation and transplant research funding. This form also serves as a gate for those transitioning their licensure from other states or Canadian provinces into New York State, ensuring compliance and facilitating the integration of drivers into New York's licensing system with ease. The complex interweaving of administrative procedure with community welfare and personal civic duty encapsulated in the MV-44EDL highlights the form's significance beyond its primary function.
| Question | Answer |
|---|---|
| Form Name | Form Mv 44Edl |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | SSN, mv44 pdffiller, mv44 form, suffix drivers license |
New York State Department of Motor Vehicles |
|
APPLICATION FOR ENHANCED DRIVER LICENSE OR |
|
PLEASE PRINT CLEARLY IN BLUE OR BLACK INK. |
|
THIS FORM IS ALSO AVAILABLE ON DMV’S WEB SITE AT: www.dmv.ny.gov |
|
IAMAPPLYING FORAN ENHANCED |
(check any that apply): |
PAGE 1 OF 3
Batch File No.
Image No.
LRC |
LAM |
LRN |
LDP |
LNO |
LIS |
LIN |
POR |
PAM |
PRN PDP |
|
|
|
|
|
|
|
|
|
|
oUpgrade Current oLearner oID |
o |
Renewal |
o |
Replacement |
o |
oNYSlicenseinexchangeforalicensefromanotherUS |
|||
DocumenttoEDL Permit |
|
card |
|
|
Change |
|
State,theDistrictofColumbiaorCanadianProvince |
||
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|||||
|
|
|
|
||||||
VOTER REGISTRATION QUESTIONS |
(Please answer “yes” or “no”.) |
|
|
|
|||||
If you are not registered to vote where you live now, would you like to apply to register, or if |
|
oYES - Complete Voter RegistrationApplication Section |
|||||||
you are changing your address, would you like the Board of Elections to be notified? |
|
||||||||
NOTE:If you do not check either box, you will be considered to have decided not to register to vote. |
tonotifytheBoardofElectionsofmychangeofaddress. |
||||||||
SIGN BELOW ♥to enroll in the NYS Department of Health’s Donate LifeSM Registry. By signing, you are certifying that you are: 18 years of age or older; consenting to donate all of your organs and tissues for transplantation, research or both; authorizing DMV to transfer your name and identifying information to DOH for enrollment in the Registry; and authorizing DOH to allow access to this information to federally regulated organ donation organizations and
♥Donor Consent Signature: ➧____________________________________________________ Date:_____________
oCheck this box to make a $1voluntary contribution to the Life...Pass It On Trust Fund. The $1 donation will be added to your total transaction fee. Acontribution to the Fund is used for organ donation and transplant research and educational projects promoting organ and tissue donation.
|
IDENTIFICATION INFORMATION |
Do you now have, or did you ever have a New York: |
NYS DRIVER LICENSE, LEARNER PERMIT, or |
|||||||||||
|
Driver license? . . . . . oYes |
oNo |
|
|
||||||||||
|
If “Yes”, enter the identification number as it appears |
|||||||||||||
|
Learner permit? . . . . oYes |
oNo |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||||
|
} on the license, learner permit, or |
|
|
|
|
|
|
|
|
|
||||
|
oNo |
|
|
|
|
|
|
|
|
|
||||
FULL LAST NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Do you have or did you ever have a driver license that is valid or |
|||||||||
|
|
|
|
|
that expired within the past year, issued by another US State, the |
|||||||||
FULL FIRST NAME |
|
|
|
|||||||||||
|
|
|
District of Columbia or a Canadian Province? oYes oNo |
|||||||||||
|
|
|
|
|
||||||||||
|
|
|
|
|
If “Yes”, where was it issued? ____________________________ |
|||||||||
|
|
|
|
|
||||||||||
FULL MIDDLE NAME |
|
Date of Expiration: |
Type of License: |
||
|
|
|
|
|
|
License ID No.:
SUFFIX |
DATE OF BIRTH |
|
|
||||
|
|
Month |
Day |
Year |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SEX
Male Female
o o
HEIGHT
Feet Inches
EYE COLOR
DAY PHONE NO. (Optional)
Area Code
()
SOCIALSECURITYNUMBER*(SSN) *YoumustprovideyourSSN.AuthoritytocollectyourSSNisgrantedbySections490.3and502oftheVehicleandTrafficLaw.
The information will be used only for exchange with other jurisdictions, to assistinverification
of identity, and to invoke driver license sanctions pursuant to V&TLaw Section
number will not be given to the public, or appear on any form or information request.
ADDRESS WHEREYOU GETYOUR MAIL - Include Street Number and Name, Rural Delivery and/or box number (If PO Box, also fill in “Address WhereYou Live” below)
|
Apt. No. |
City or Town |
State |
|
Zip Code |
County |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS WHEREYOU LIVE REQUIRED IFDIFFERENT FROM MAILINGADDRESS - DO NOT GIVE P.O. BOX. THISADDRESS WILLAPPEAR ONYOUR DRIVER LICENSE. |
||||||
|
Apt. No. |
City or Town |
State |
|
Zip Code |
County |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Has your name changed? oYes oNo |
|
|
|
|
Has your mailing address changed? |
|
Has the address where you live changed? oYes oNo |
||||||||||||||||||||||||||||||||||||
If “Yes”, print your former name exactly as it |
|
|
|
|
|
|
|
|
oYes oNo |
|
|
|
|
|
What is the change and the reason for it |
||||||||||||||||||||||||||||
OTHER CHANGE: |
|
||||||||||||||||||||||||||||||||||||||||||
appears on your present license or |
|
|
|
||||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(new license class, wrong date of birth, etc.)? |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PLEASE COMPLETEAND SIGN PAGE 2. |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
F |
Other |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
License |
|
|
A |
B |
C |
|
D |
DJ |
|||||||
O |
Restrictions |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Class |
|
|
|
E |
ID |
M |
|
|
MJ |
|||||||
R |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
Endorsements |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Special |
|
|
AM |
PP |
DP |
LR |
|
LS |
BC |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
O |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
RestrictionsVehicle |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Conditions |
|
ML |
NF |
UC |
UP |
UR |
X8 |
XT |
||||||||||||||
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
STOP/RESPONSE |
|
|
|
|
|
|
|
|
Proof Submitted: oBirth Certificate |
oDriver License/ID |
Approved By |
|
|
Date |
|||||||||||||||||||||||||||||
I |
|
|
|
|
|||||||||||||||||||||||||||||||||||||||
CE |
oFailed to answer summons |
oTEENS |
|
oPassport oLearner Permit |
oResidency |
|
oCredit Card |
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
U |
oInsurance lapse |
|
|
|
|
|
|
|
|
oImage Retrieval oSocial Security Card oMedical Certificate (CDL only) Office |
|
|
|
|
|
|
|||||||||||||||||||||||||||
|
|
Other: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||
S |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EoLicense/Permit Surrendered for
PAGE 2 OF 3 |
||||
|
|
|
|
|
|
|
|
||
|
DRIVER LICENSE and LEARNER PERMIT APPLICANTS ONLY |
|
|
|
|
1. Have you had, or are you being treated for, any of the following, or has a previous disability worsened? o Yes |
o No If “Yes”, check all that apply. |
||
|
o 1. Convulsive disorder, epilepsy, fainting or dizzy spells, or any condition which causes unconsciousness |
|
||
|
o 2. |
Heart ailment |
|
|
|
o 3. |
Hearing impairment |
|
|
|
o 4. |
Lost use of leg, arm, foot, hand, or eye |
|
|
|
o 5. |
Other (explain)___________________________________________________________________________________________________________ |
||
If you checked box 1, you and your doctor must complete form
2.Have you had a driver license, learner permit, or privilege to operate a motor vehicle suspended, revoked or cancelled, or an application for a license
denied in this state or elsewhere, in this or any other name? o Yes o No
If “Yes”, has your license, permit or privilege been restored, or your application approved? o Yes o No
oJunior License
I am the parent or guardian of the applicant, and I consent to the issuance of a learner permit, license or (if under 16) a
Parent or Guardian
Sign Here ➧
Teen Electronic Event Notification Service (TEENS)
I would like to enroll in the TEENS program to be notified if the under 18
(Relationship toApplicant) |
(Date) |
COMMERCIAL DRIVER LICENSEAPPLICANTS ONLY Please answer questions 1 & 2, below:
1. |
Did you have a driver license from the District of Columbia or any US state, otherthanNewYork, in the past 10 years? o Yes o No |
|
If YES, list the names of all of the states or DC, but if you are turning in a license from another state, do notlist that state: |
2. |
Do you certify that you comply with federal requirements set forth in 49 CFR Part 391 and have a valid Medical Examiner’s Certificate? o Yes o No |
|
If YES, you must present your Medical Certificate to prove you meet this standard. |
|
If NO, will your commercial driving be limited to municipal and/or school operations only? o Yes o No |
NOTE: For an explanation of 49 CFR 391 requirements and operations that do not require a Medical Examiner’s Certificate, see form
CERTIFICATION I certify that the information I have given on this application is true. I certify that I am a citizen of the United States ofAmerica and a resident of New York State. If I am applying for a replacement license or
I understand that the information and documentation that I have provided in connection with this application will be used to verify my identity, New York State residency and United States citizenship. I understand that this information and documentation will be shared with the New York State and United States federal entities for these verification purposes and I consent to this dissemination and use.
IMPORTANT: Making a false statement in any license or
SIGN HERE ➧
PLEASE
NAME ➧
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CREDIT CARDAUTHORIZATION IF CARDHOLDER IS NOT THEAPPLICANT: |
|
|
|
|
|
|
|||||
|
My signature authorizes____________________________________________ |
Sign |
|
|
|
|
||||||
|
Here ➧ |
|
|
|
|
|||||||
|
to use my credit card for payment of any fees in connection with this application and I |
|
|
|
|
|||||||
|
|
|||||||||||
|
understand that I must be present for this transaction. |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|||
|
O |
|
TEST RESULTS |
|
|
|
Applicant’s Signature |
|
Examiner’s Initials |
|||
|
F |
U |
|
|
|
|
|
|
|
|
|
|
|
F |
S |
Eye |
o Pass |
o Corrective Lens |
1 |
|
|
|
|
|
|
|
I |
E |
|
|
|
|
|
|
|
|
|
|
|
C |
|
|
|
|
|
|
|
|
|
|
|
|
E |
|
Written |
o Pass |
o Fail |
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PAGE 3 OF 3
NEW YORK STATE VOTER REGISTRATIONAPPLICATION INFORMATION |
OFFICE USE ONLY |
||
|
(Please read before you complete application on the other side.) |
|
|
You Can Use This Form To: |
To Register You Must: |
|
|
|
|||
register to vote in New York State |
be a U.S. citizen |
|
|
change your name and/or address, if there is a change since you voted |
be 18 years old by December 31 of the year in which you file this form |
|
enroll in a political party or change your enrollment |
||
(note: you must be 18 years old by the date of the general, primary or |
||
|
||
|
other election in which you want to vote.) |
|
|
live in the county, city, or village, at least 30 days before an election |
|
|
not be in jail or on parole for a felony conviction |
|
|
not claim the right to vote elsewhere |
If you would like help in filling out the voter registration application form, we will help you. The decision whether to seek or accept help is yours. You may fill out the application form in private.
If you believe that someone has interfered with your right to register or decline to register to vote, your right to privacy in deciding whether to register or in applying to register to vote, or your right to choose your own political party or other political preference, you may file a complaint with the NYS Board of Elections, 40 Steuben Street,Albany, NY
If you have any questions about registering to vote, you should call your County Board of Elections or call
NEW YORK STATE VOTER REGISTRATIONAPPLICATION - (Fill out this part only if you want to register to vote or change your address or other information with the Board of Elections, and if you are also filling out the DMV application above.)
If you register to vote, your completed voter registration application will be sent directly to the Board of Elections. If you decline to register, your decision will remain confidential. You will be notified by your County Board of Elections when your voter registration application has been processed.
Are you a U.S. citizen? o Yes |
o No |
|
I will be 18 years old on or before election day: |
o Yes o No |
Home Telephone Number (optional) |
||||||||||||
If you answered NO, do not complete this form. |
|
If you answered NO, do not complete this form, unless you will be 18 by the end of the year. |
Area Code |
||||||||||||||
|
( |
) |
|||||||||||||||
Last year voted |
YourAddress was (give house number, street, and city) |
|
In county/state |
Under the name (if different from your name now) |
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Choose a Party – Check one box only |
|
AFFIDAVIT: I swear or affirm that |
|
|
|
|
|
||||||||||
o DEMOCRATIC PARTY |
|
|
Please note: In order |
|
I am a citizen of the United States. |
|
|
||||||||||
|
|
|
I will have lived in the county, city, or village for at least 30 days before the election. |
|
|||||||||||||
o REPUBLICAN PARTY |
|
to vote in a primary |
|
|
|||||||||||||
|
|
I meet all requirements to register to vote in New York State. |
|
|
|||||||||||||
|
|
|
|
|
election, you must be |
|
|
|
|||||||||
o CONSERVATIVE PARTY |
|
|
This is my signature or mark on the line below. |
|
|
||||||||||||
|
enrolled in a party. |
|
|
|
|
||||||||||||
o WORKINGFAMILIESPARTY |
|
|
|
The above information is true. I understand that if it is not true I can be convicted and fined up to $5,000 and/or |
|||||||||||||
|
*Except the Independence |
|
|||||||||||||||
|
|
|
|
|
|
jailed for up to four years. |
|
|
|
|
|
||||||
o INDEPENDENCE PARTY* |
|
Party which permits non- |
|
|
|
|
|
|
|||||||||
|
|
|
↓ Signature or mark |
↓ |
|
|
|||||||||||
o GREEN PARTY |
|
|
|
|
enrolled voters to vote in |
|
|
|
|
||||||||
|
|
|
|
their primary election. |
|
|
|
|
|
|
|
|
|
|
|||
o OTHER(writein) _______________________ |
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||
o I DO NOT WISH TO ENROLL INAPARTY |
|
X |
|
|
|
|
|
Date |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|