
With the online tool for PDF editing by FormsPal, you'll be able to fill in or alter conditional license here and now. The editor is consistently maintained by us, receiving handy features and growing to be greater. Starting is effortless! Everything you need to do is take these basic steps down below:
Step 1: Click on the "Get Form" button above on this page to get into our PDF editor.
Step 2: With the help of our advanced PDF tool, it is possible to accomplish more than merely fill out forms. Express yourself and make your forms seem faultless with custom text put in, or optimize the file's original input to perfection - all comes with the capability to incorporate stunning images and sign the PDF off.
Pay attention when completing this document. Make certain all necessary areas are filled out correctly.
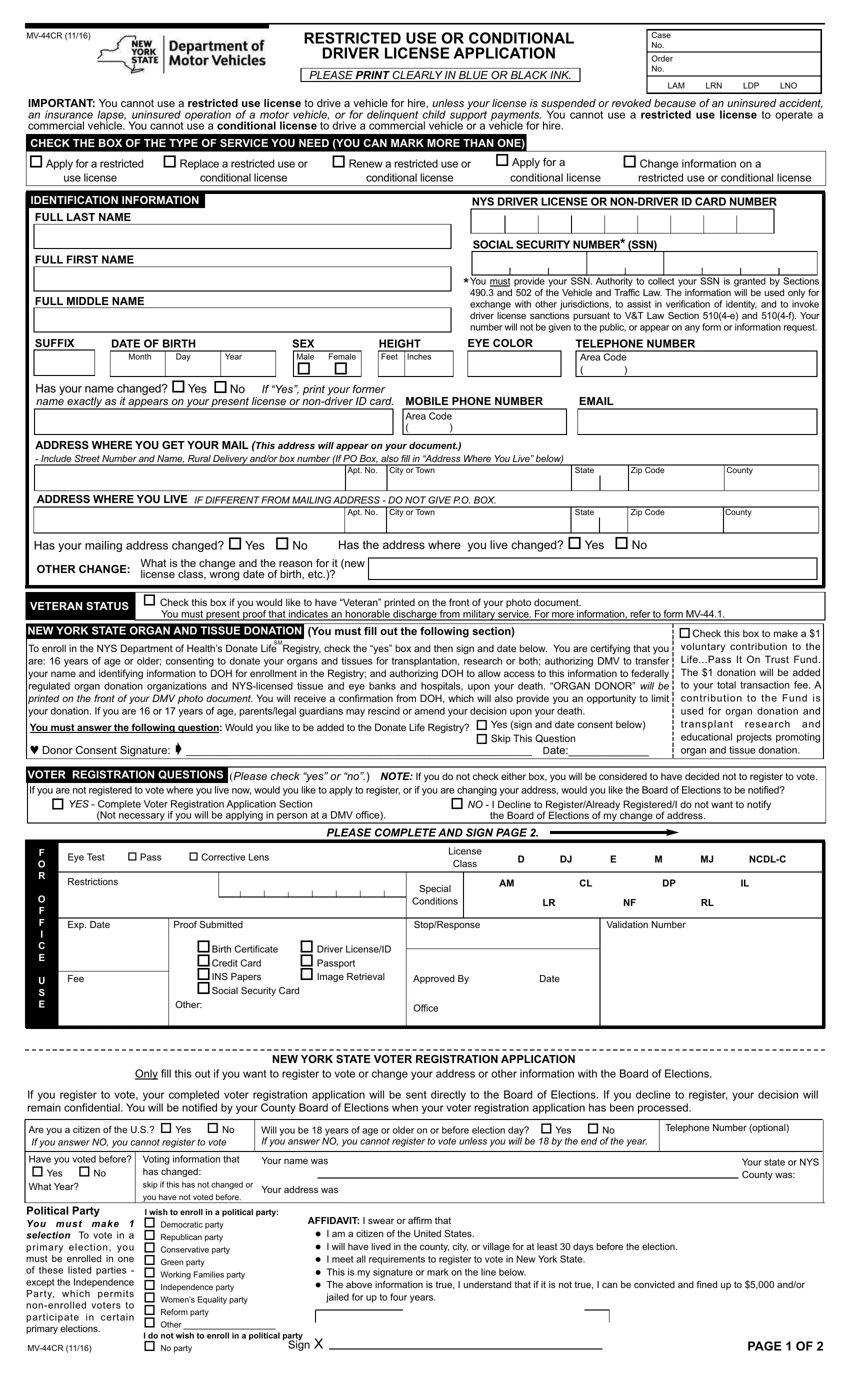
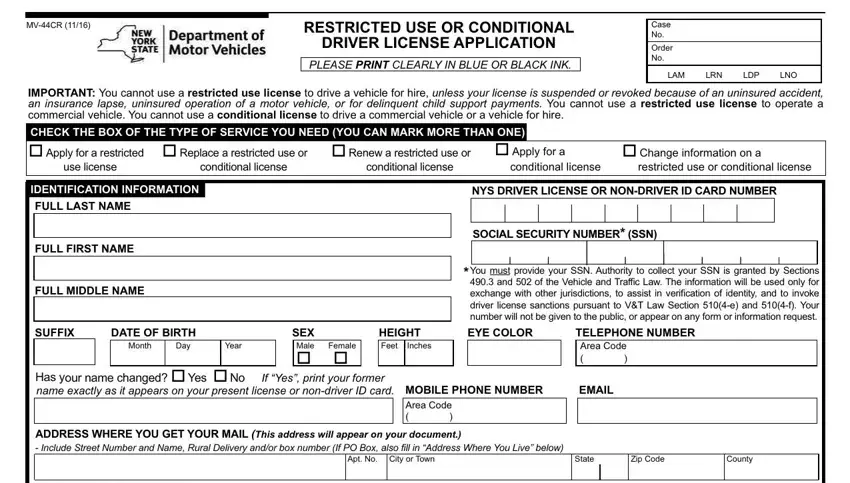
1. When filling in the conditional license, ensure to complete all essential blank fields in the relevant area. It will help facilitate the process, enabling your information to be handled swiftly and properly.
2. Just after performing this section, go to the subsequent step and complete all required particulars in all these fields - ADDRESS WHERE YOU LIVE, IF DIFFERENT FROM MAILING ADDRESS, Apt No City or Town, State, Zip Code, County, Has your mailing address changed o, Has the address where you live, OTHER CHANGE, What is the change and the reason, VETERAN STATUS, Check this box if you would like, NEW YORK STATE ORGAN AND TISSUE, You must fill out the following, and To enroll in the NYS Department of.
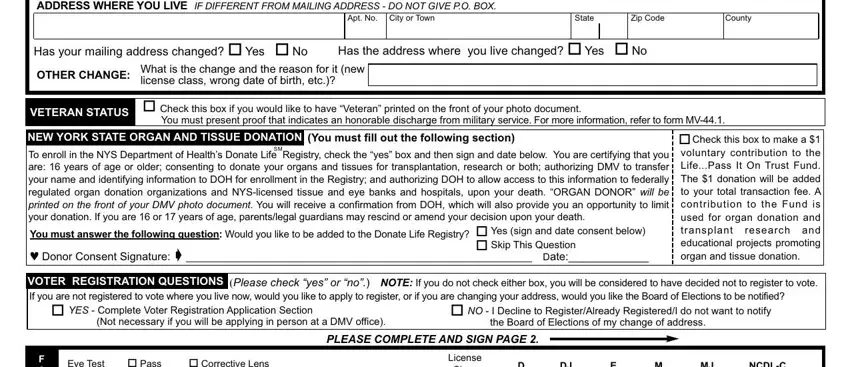
Be very careful when completing VETERAN STATUS and You must fill out the following, as this is the part in which many people make mistakes.
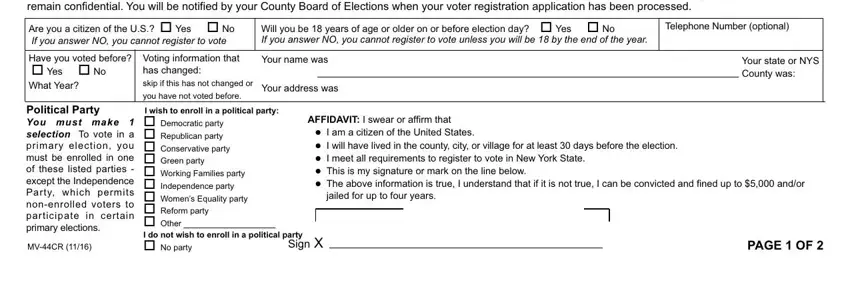
3. Within this part, review If you register to vote your, Are you a citizen of the US o Yes, Will you be years of age or older, Telephone Number optional, Have you voted before o Yes o No, Voting information that has, you have not voted before, Your name was, Your address was, Your state or NYS County was, Political Party You must make, MVCR, I wish to enroll in a political, AFFIDAVIT I swear or affirm that, and Sign. Each of these will have to be filled in with highest accuracy.
4. Completing Have you had or are you currently, Do you need a hearing aid andor, Have you lost use of a leg arm, CERTIFICATION I certify that the, IMPORTANT Making a false statement, SIGN HERE, and DATE is vital in this part - don't forget to take your time and fill out every single empty field!
Step 3: Before submitting your form, check that all form fields have been filled out the proper way. As soon as you’re satisfied with it, press “Done." Obtain your conditional license the instant you join for a 7-day free trial. Easily get access to the pdf form inside your FormsPal cabinet, with any edits and changes all synced! At FormsPal.com, we strive to be sure that your details are kept private.