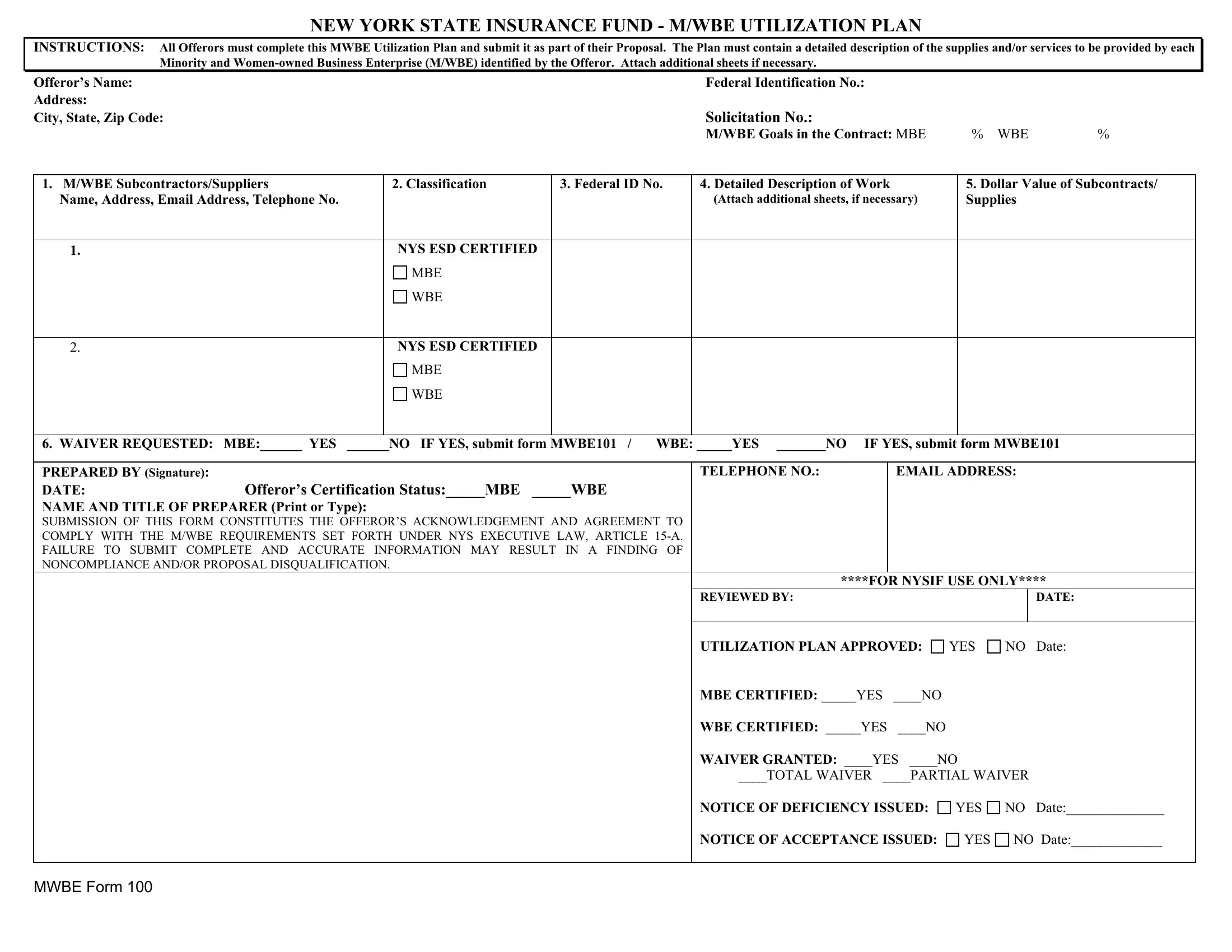
In New York State, fostering diversity and inclusion within the business sector is not just an ethical imperative but a formalized process, clearly delineated through mechanisms like the MWBE (Minority and Women-owned Business Enterprises) Utilization Plan, encapsulated in the MWBE 100 form. This detailed document serves as a critical component for Offerors intending to participate in contracts involving the state's insurance fund. It mandates a comprehensive outline of how these businesses plan to integrate certified minority and women-owned suppliers and subcontractors into their proposals, including providing their identification numbers, services, or supplies to be delivered, and the financial scope of their involvement. The form also opens a pathway for requests for waivers, should meeting the set participation goals prove challenging, while simultaneously binding Offerors to adhere to New York State Executive Law, Article 15-A, underpinning the state's commitment to economic equality and opportunity. It's an intricate balance between ensuring fair participation and maintaining the standard of service delivery, with failure to comply or to provide accurate, complete information potentially leading to proposal disqualification or a finding of noncompliance. Such measures underscore New York's strategic approach to nurturing an inclusive economic environment, promoting not just diversity in business ownership but ensuring these enterprises have a tangible role in the state's economic activities.
| Question | Answer |
|---|---|
| Form Name | Mwbe Form 100 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | utilization report sample, fund utilization report sample excel, budget utilization report sample, funds utilisation report format |
NEW YORK STATE INSURANCE FUND - M/WBE UTILIZATION PLAN
INSTRUCTIONS: All Offerors must complete this MWBE Utilization Plan and submit it as part of their Proposal. The Plan must contain a detailed description of the supplies and/or services to be provided by each Minority and
Offeror’s Name: |
|
|
|
|
|
Federal Identification No.: |
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
City, State, Zip Code: |
|
|
|
|
|
Solicitation No.: |
|
|
|
|
|
|
|
|
|
|
|
|
|
M/WBE Goals in the Contract: MBE |
% |
WBE |
% |
||||
|
|
|
|
|
|
|
|
|
|
|
|||
1. M/WBE Subcontractors/Suppliers |
|
2. Classification |
|
3. Federal ID No. |
4. Detailed Description of Work |
|
|
5. Dollar Value of Subcontracts/ |
|||||
Name, Address, Email Address, Telephone No. |
|
|
|
|
(Attach additional sheets, if necessary) |
|
Supplies |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1. |
|
|
NYS ESD CERTIFIED |
|
|
|
|
|
|
|
|
|
|
|
|
|
MBE |
|
|
|
|
|
|
|
|
|
|
|
|
|
WBE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. |
|
|
NYS ESD CERTIFIED |
|
|
|
|
|
|
|
|
|
|
|
|
|
MBE |
|
|
|
|
|
|
|
|
|
|
|
|
|
WBE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
6. WAIVER REQUESTED: MBE:______ YES |
______NO IF YES, submit form MWBE101 / WBE: _____YES _______NO IF YES, submit form MWBE101 |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|||
PREPARED BY (Signature): |
|
|
|
|
|
TELEPHONE NO.: |
|
EMAIL ADDRESS: |
|
||||
DATE: |
Offeror’s Certification Status:_____MBE |
_____WBE |
|
|
|
|
|
|
|
|
|||
NAME AND TITLE OF PREPARER (Print or Type): |
|
|
|
|
|
|
|
|
|
|
|||
SUBMISSION OF THIS FORM CONSTITUTES THE OFFEROR’S ACKNOWLEDGEMENT AND AGREEMENT TO |
|
|
|
|
|
|
|
|
|||||
COMPLY WITH THE M/WBE REQUIREMENTS SET FORTH UNDER NYS EXECUTIVE LAW, ARTICLE |
|
|
|
|
|
|
|
|
|||||
FAILURE TO SUBMIT COMPLETE AND ACCURATE INFORMATION MAY RESULT IN A FINDING OF |
|
|
|
|
|
|
|
|
|||||
NONCOMPLIANCE AND/OR PROPOSAL DISQUALIFICATION. |
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
****FOR NYSIF USE ONLY**** |
|||||||
|
|
|
|
|
|
REVIEWED BY: |
|
|
|
|
|
DATE: |
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
UTILIZATION PLAN APPROVED: |
YES |
NO |
DATE: |
||||
|
|
|
|
|
|
MBE CERTIFIED: _____YES |
____NO |
|
|
|
|
|
|
|
|
|
|
|
|
WBE CERTIFIED: _____YES |
____NO |
|
|
|
|
|
|
|
|
|
|
|
|
WAIVER GRANTED: ____YES ____NO |
|
|
|
||||
|
|
|
|
|
|
____TOTAL WAIVER ____PARTIAL WAIVER |
|
||||||
NOTICE OF DEFICIENCY ISSUED:
YES
NO DATE:______________
NOTICE OF ACCEPTANCE ISSUED:
YES
NO DATE:_____________
MWBE FORM 100