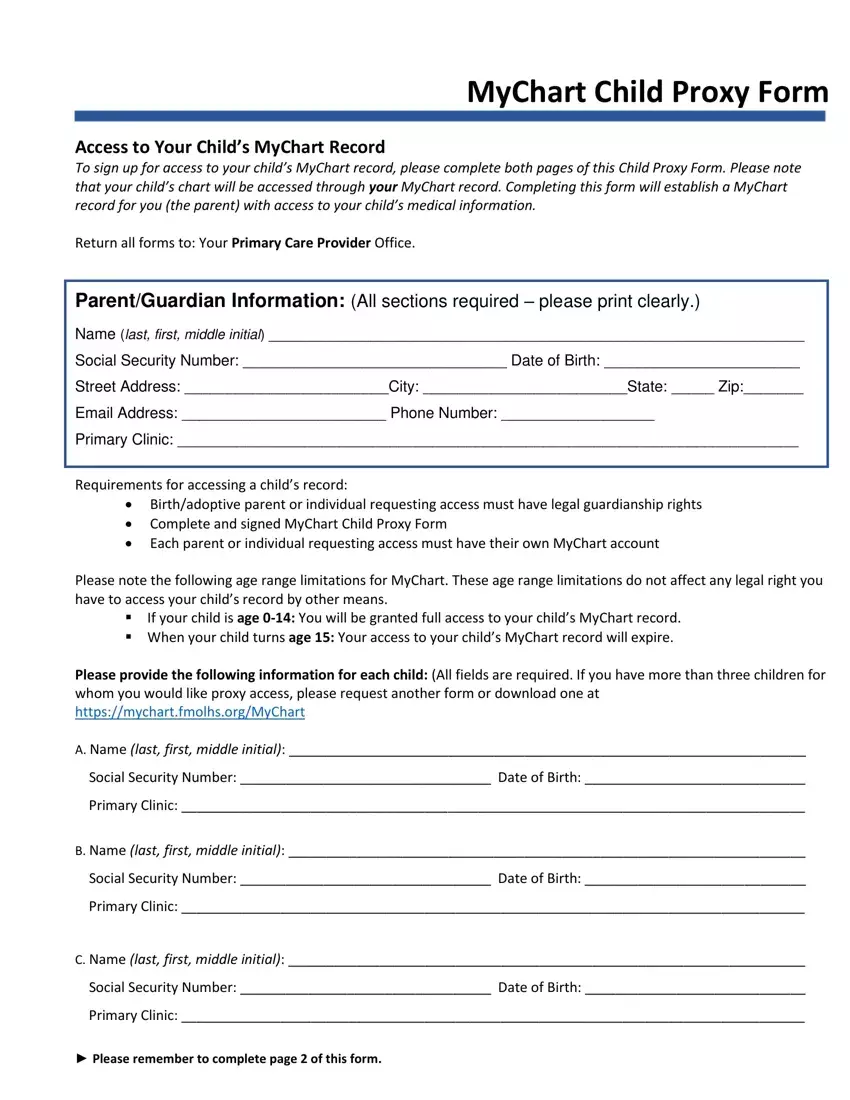
MyChart Child Proxy Form
Access to Your Child’s MyChart Record
To sign up for access to your child’s MyChart record, please complete both pages of this Child Proxy Form. Please note that your child’s chart will be accessed through your MyChart record. Completing this form will establish a MyChart record for you (the parent) with access to your child’s medical information.
Return all forms to: Your Primary Care Provider Office.
Parent/Guardian Information: (All sections required – please print clearly.)
Name (last, first, middle initial) _______________________________________________________________
Social Security Number: _______________________________ Date of Birth: _______________________
Street Address: ________________________City: ________________________State: _____ Zip:_______
Email Address: ________________________ Phone Number: __________________
Primary Clinic: _________________________________________________________________________
Requirements for accessing a child’s record:
Birth/adoptive parent or individual requesting access must have legal guardianship rights
Complete and signed MyChart Child Proxy Form
Each parent or individual requesting access must have their own MyChart account
Please note the following age range limitations for MyChart. These age range limitations do not affect any legal right you have to access your child’s record by other means.
If your child is age 0-14: You will be granted full access to your child’s MyChart record.
When your child turns age 15: Your access to your child’s MyChart record will expire.
Please provide the following information for each child: (All fields are required. If you have more than three children for whom you would like proxy access, please request another form or download one at https://mychart.fmolhs.org/MyChart
A. Name (last, first, middle initial): ____________________________________________________________________
Social Security Number: _________________________________ Date of Birth: _____________________________
Primary Clinic: __________________________________________________________________________________
B. Name (last, first, middle initial): ____________________________________________________________________
Social Security Number: _________________________________ Date of Birth: _____________________________
Primary Clinic: __________________________________________________________________________________
C. Name (last, first, middle initial): ____________________________________________________________________
Social Security Number: _________________________________ Date of Birth: _____________________________
Primary Clinic: __________________________________________________________________________________
►Please remember to complete page 2 of this form.
MyChart Child Proxy Form (page 2)
MyChart Terms and Agreement
By signing below, I acknowledge that I have read, understand, and agree to the MyChart Terms and Conditions.
A copy of the MyChart Terms and Conditions can be requested at your physician’s office and can be obtained online at https://mychart.fmolhs.org/MyChart
►___________________/___________/___________/_______
Signature of Parent/Guardian |
Relationship to Patient |
Date |
Time |