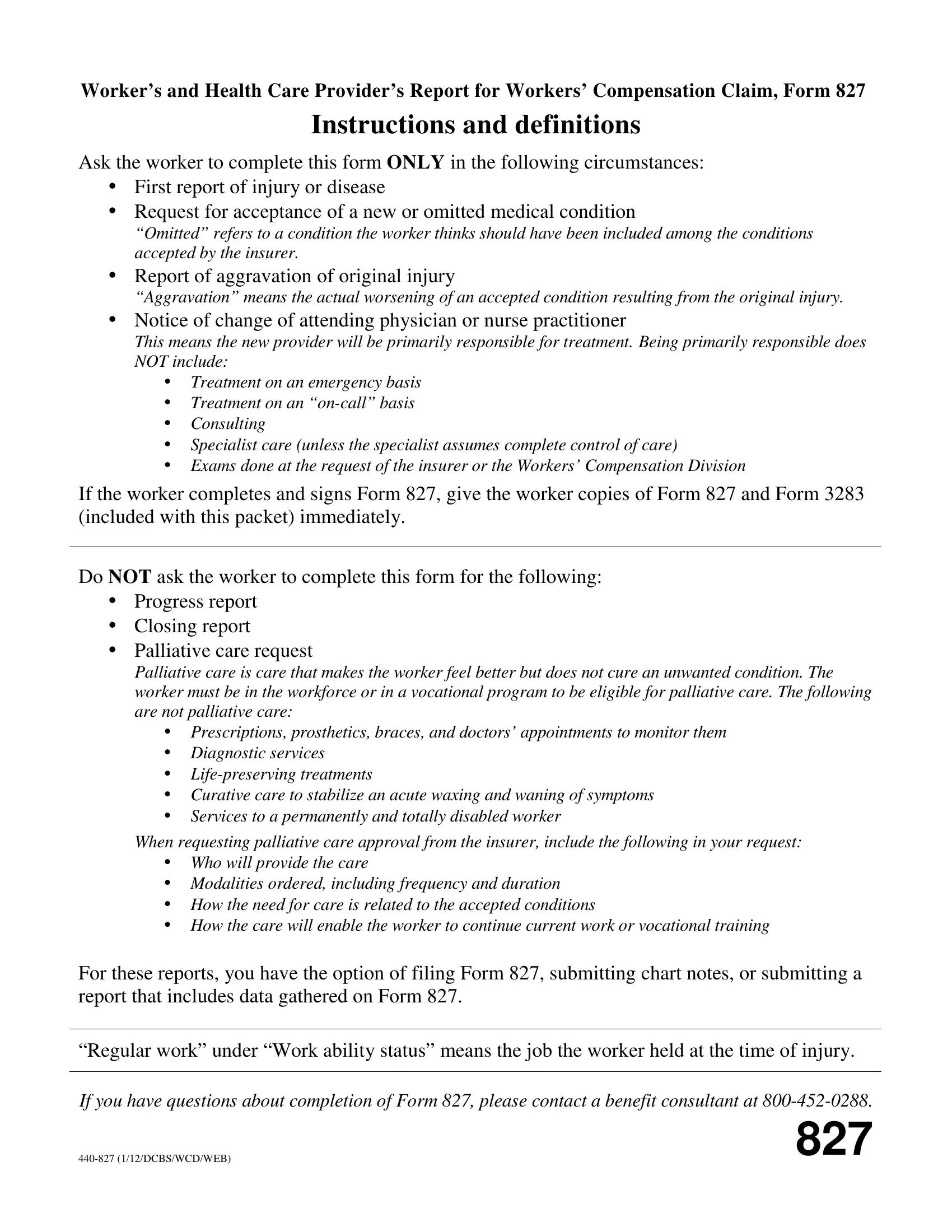
Navigating the complexities of workers' compensation claims can be a daunting task for both workers and healthcare providers. The Mylakerlink form, formally known as the Worker’s and Health Care Provider’s Report for Workers’ Compensation Claim, Form 827, plays a crucial role in this process. This document is designed exclusively for instances such as the initial report of injury or disease, requests for the acceptance of new or omitted medical conditions, reports of aggravation of an original injury, and notices regarding changes in the attending physician or nurse practitioner. Its purpose is to streamline the communication between injured workers, healthcare providers, and insurers, ensuring that all parties are accurately informed about the case at hand. The form requires detailed information about the worker's situation, including personal details, the nature of the injury or disease, and the treatment required. Additionally, it includes a section for healthcare providers to fill out, which covers diagnostic codes, treatment plans, and work ability status. With instructions on how both workers and healthcare providers should complete and submit this form, it serves as a guide to expedite the workers’ compensation process, aiming to assist workers in receiving the appropriate care and support they need following a workplace injury.
| Question | Answer |
|---|---|
| Form Name | Mylakerlink Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | how to 827, 827, 827 form, workers compensation form 827 |
