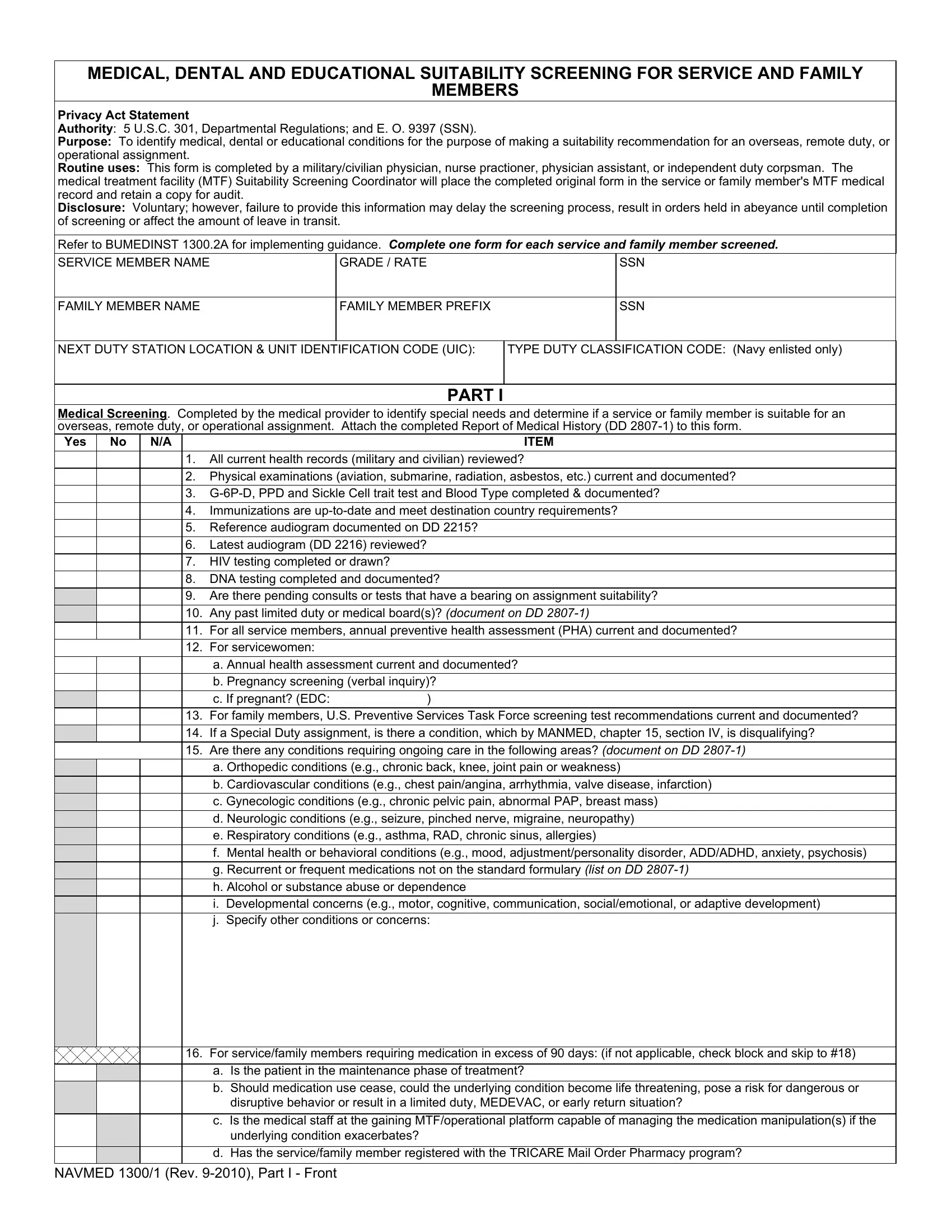
The NAVMED 1300 form is an essential document used in the United States Navy, serving a crucial role in assessing the medical, dental, and educational suitability of service members and their families for overseas, remote duty, or operational assignments. Mandated by 5 U.S.C. 301, Departmental Regulations, and Executive Order 9397 (SSN), the form facilitates a comprehensive screening process to identify any medical, dental, or educational conditions that might influence the suitability recommendation for such assignments. This rigorous screening is conducted by qualified professionals including military/civilian physicians, nurse practitioners, physician assistants, or independent duty corpsmen. These professionals ensure that the form, along with the attached Report of Medical History (DD 2807-1), thoroughly documents a variety of assessments - from reviewing all current health and dental records to validating the completion of crucial tests such as HIV, DNA, and immunizations that meet destination country requirements. Additionally, it addresses the need for special medical supplies, adaptive equipment, and the potential requirement for ongoing care in areas encompassing orthopedic, cardiovascular, gynecologic, neurologic, respiratory conditions, and more. The NAVMED 1300 form also incorporates a detailed dental screening section, crucial for determining the dental class of the service member and ensuring that their dental needs align with the capabilities of the medical treatment facilities at the gaining location. This meticulous process, while voluntary, is critical, as failure to provide complete and accurate information can delay the screening process, affecting the assignment of orders and the overall transition for service and family members.
| Question | Answer |
|---|---|
| Form Name | Navmed 1300 Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | navmed 1300 1 pdf fillable, navmed 1300 2, audiogram, navmed 1300 1 pdf |