

With the help of the online PDF editor by FormsPal, it is possible to complete or change Nc Form 33 here. FormsPal professional team is always working to develop the editor and make it much easier for people with its multiple functions. Take your experience to another level with constantly growing and exciting options we provide! To get the process started, go through these simple steps:
Step 1: Press the "Get Form" button above. It is going to open our tool so you could start filling in your form.
Step 2: Once you open the editor, you will notice the document made ready to be filled in. Besides filling out different blanks, you might also do other actions with the file, specifically adding custom textual content, editing the original textual content, adding graphics, affixing your signature to the document, and more.
This PDF form requires particular information to be filled in, so you should definitely take the time to type in what is asked:
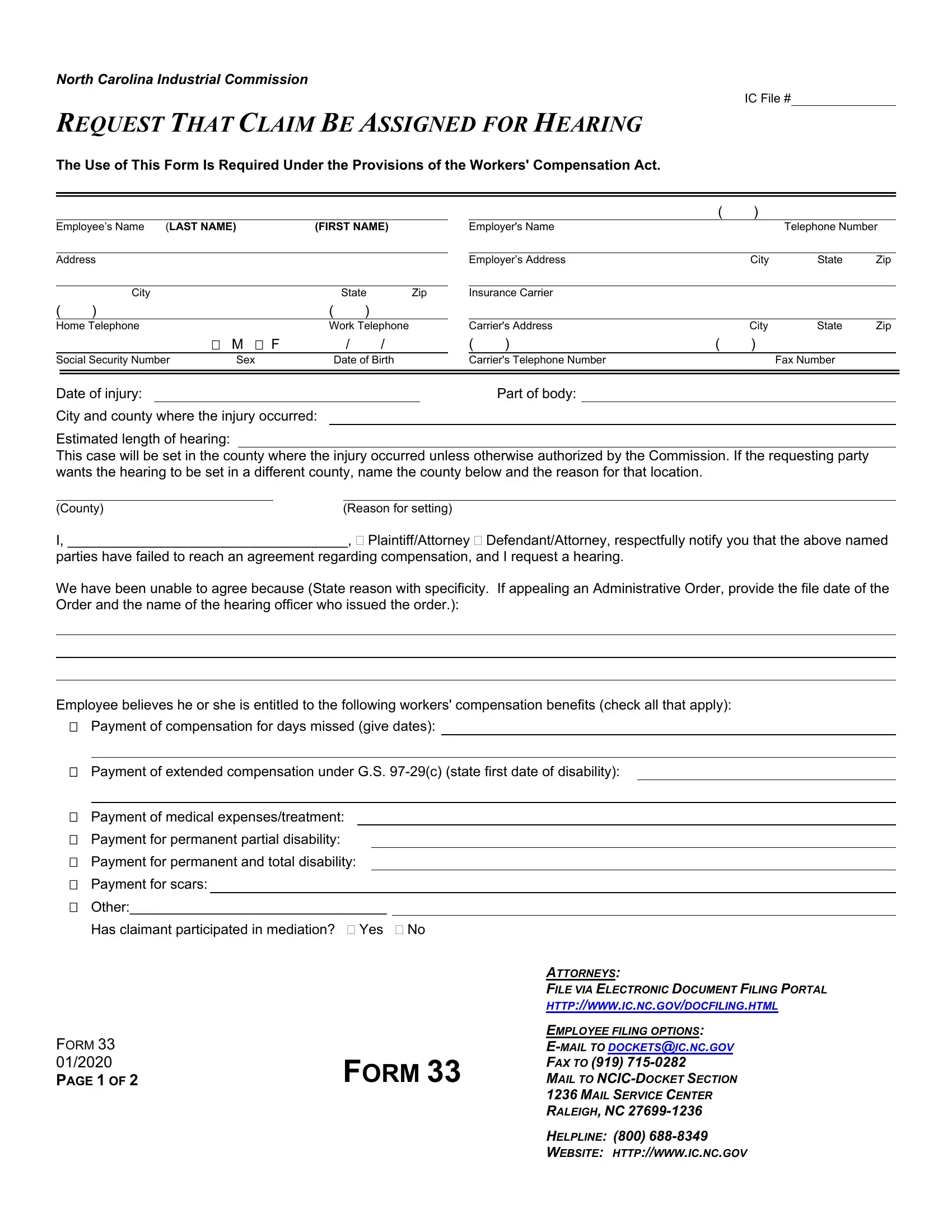
1. Start completing the Nc Form 33 with a group of necessary fields. Note all of the required information and ensure there is nothing forgotten!
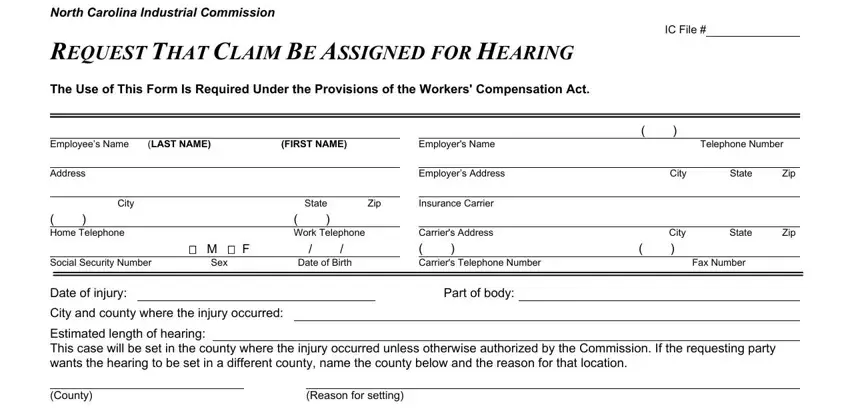
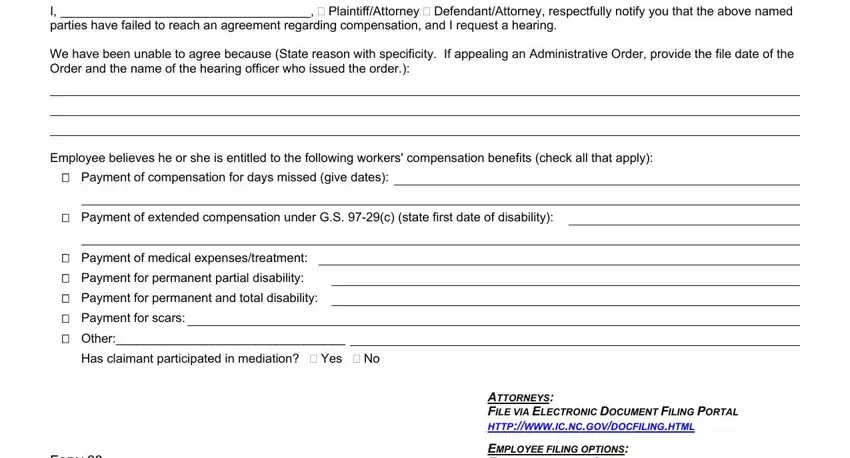
2. Once your current task is complete, take the next step – fill out all of these fields - County I PlaintiffAttorney, Employee believes he or she is, Payment of compensation for days, Payment of extended compensation, Payment of medical, ATTORNEYS FILE VIA ELECTRONIC, and FORM PAGE OF with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. This third stage will be straightforward - fill in all of the fields in NAME, ADDRESS, I hereby certify that this case is, send me signed subpoenas for my, Signature of Party Requesting, Check one Employee Employer, Printed Name of Party Requesting, Telephone Number, Email Address, Mailing Address Street and number, Date of Notice, and Notice to Employees The original to conclude this part.
Always be really attentive when completing I hereby certify that this case is and NAME, as this is the section where a lot of people make some mistakes.
4. The following subsection needs your attention in the subsequent areas: CERTIFICATE OF SERVICE, I hereby certify that on I served, supporting documents on the, US Mail special delivery mail, Note List name and address of each, ATTORNEYS FILE VIA ELECTRONIC, FORM, and FORM PAGE OF. Ensure that you type in all of the requested information to go forward.
Step 3: As soon as you've reviewed the details provided, just click "Done" to finalize your form at FormsPal. Right after getting a7-day free trial account here, it will be possible to download Nc Form 33 or send it via email without delay. The PDF document will also be readily accessible from your personal account page with your each modification. FormsPal provides secure form editing with no personal data recording or any sort of sharing. Rest assured that your data is in good hands here!