

In case you wish to fill out doh medical form nyc, it's not necessary to download and install any sort of applications - simply make use of our online PDF editor. FormsPal team is committed to providing you the ideal experience with our tool by continuously presenting new capabilities and upgrades. Our tool has become even more intuitive as the result of the most recent updates! At this point, filling out PDF forms is a lot easier and faster than ever. To get the process started, consider these easy steps:
Step 1: Access the PDF file in our editor by clicking the "Get Form Button" in the top area of this page.
Step 2: The editor enables you to work with PDF forms in various ways. Transform it by including customized text, adjust what is originally in the file, and include a signature - all within a couple of mouse clicks!
With regards to the blanks of this particular document, this is what you want to do:
1. Whenever completing the doh medical form nyc, be sure to incorporate all of the needed blanks within the corresponding form section. It will help facilitate the process, enabling your details to be processed without delay and properly.
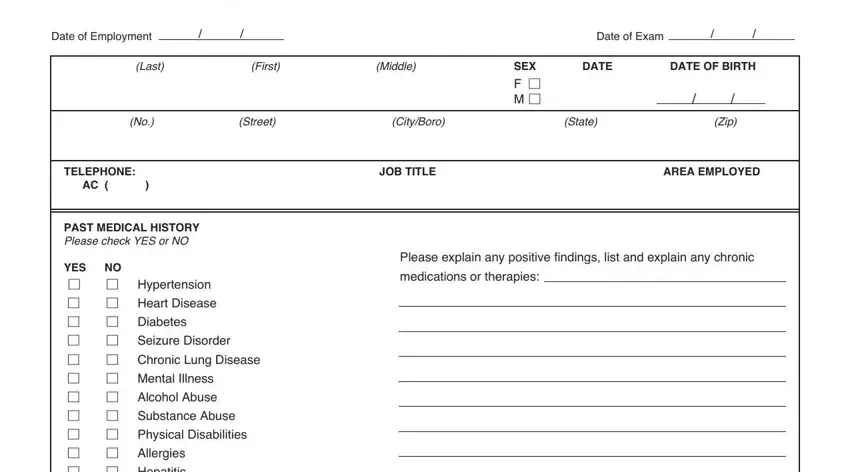
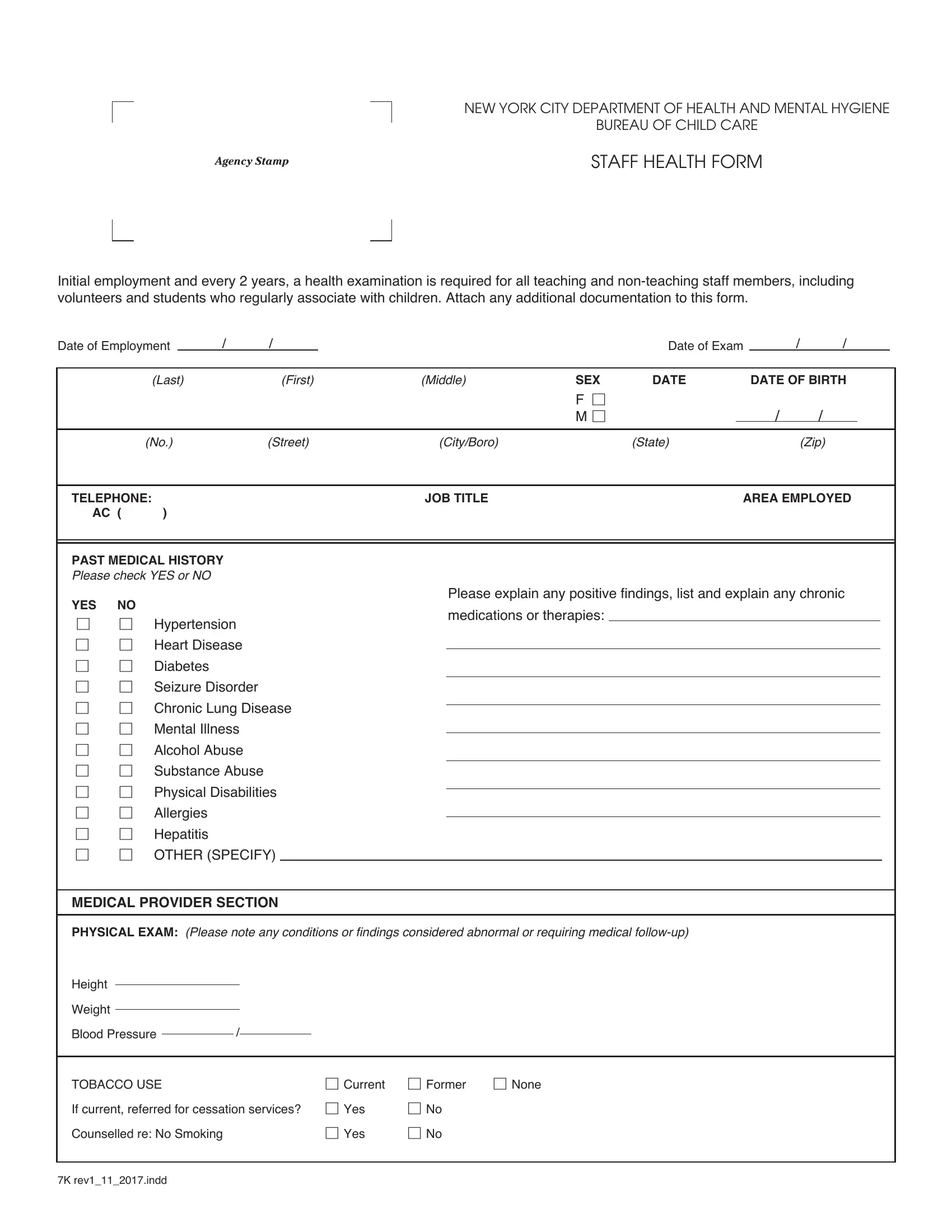
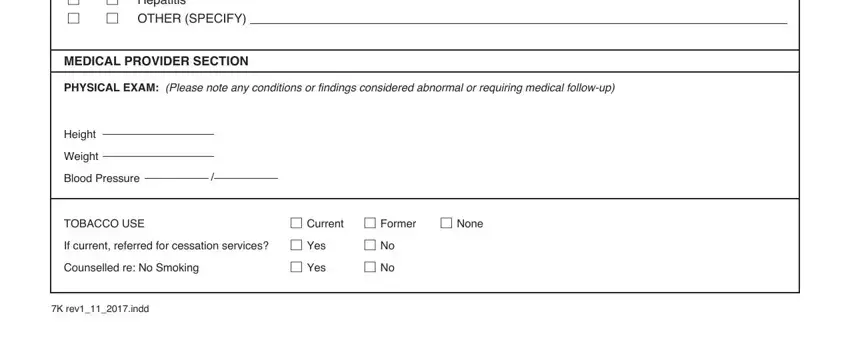
2. Once your current task is complete, take the next step – fill out all of these fields - YES NO M M Hypertension M M Heart, MEDICAL PROVIDER SECTION, PHYSICAL EXAM Please note any, Height, Weight, Blood Pressure, TOBACCO USE If current referred, Counselled re No Smoking, M No M No, M Current M Former M None, and K revindd with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
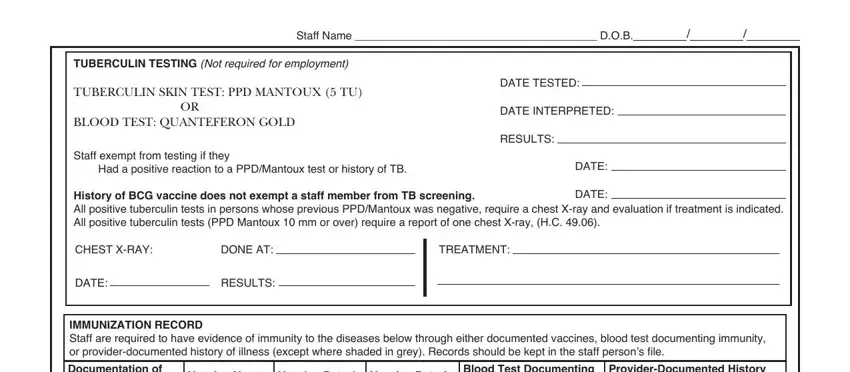
3. The next part is generally easy - fill out all the form fields in Staff Name DOB, TUBERCULIN TESTING Not required, TUBERCULIN SKIN TEST PPD MANTOUX, Staff exempt from testing if they, DATE TESTED, DATE INTERPRETED, RESULTS, DATE, History of BCG vaccine does not, DATE, CHEST XRAY, DONE AT, TREATMENT, DATE, and RESULTS to complete this part.
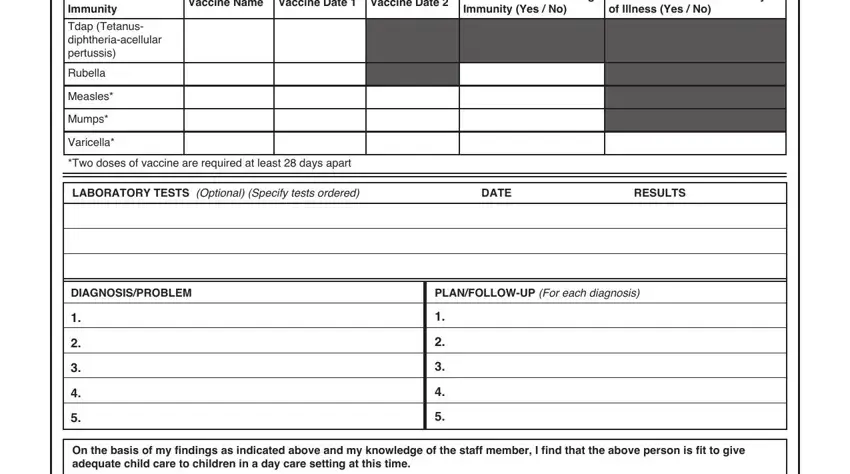
4. This next section requires some additional information. Ensure you complete all the necessary fields - IMMUNIZATION RECORD Staff are, ProviderDocumented History of, Blood Test Documenting Immunity, Vaccine Name Vaccine Date Vaccine, Tdap Tetanus diphtheriaacellular, Rubella, Measles, Mumps, Varicella, Two doses of vaccine are required, LABORATORY TESTS Optional Specify, DATE, RESULTS, DIAGNOSISPROBLEM, and PLANFOLLOWUP For each diagnosis - to proceed further in your process!
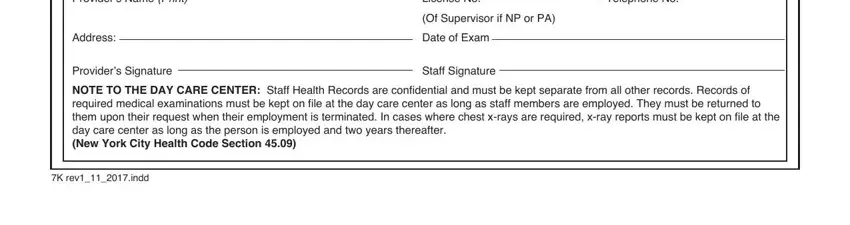
5. Lastly, this final subsection is precisely what you should wrap up before using the PDF. The blank fields in question include the following: Providers Name Print, Address, License No, Telephone No, Of Supervisor if NP or PA, Date of Exam, Providers Signature NOTE TO THE, Staff Signature, and K revindd.
Lots of people frequently get some points incorrect when completing License No in this part. You need to re-examine everything you type in right here.
Step 3: Before moving on, ensure that blanks were filled out properly. The moment you’re satisfied with it, click “Done." After creating a7-day free trial account with us, it will be possible to download doh medical form nyc or send it through email at once. The file will also be accessible in your personal cabinet with your each and every change. FormsPal ensures your information confidentiality by using a secure system that in no way records or shares any sort of sensitive information used. Rest assured knowing your paperwork are kept confidential any time you work with our services!