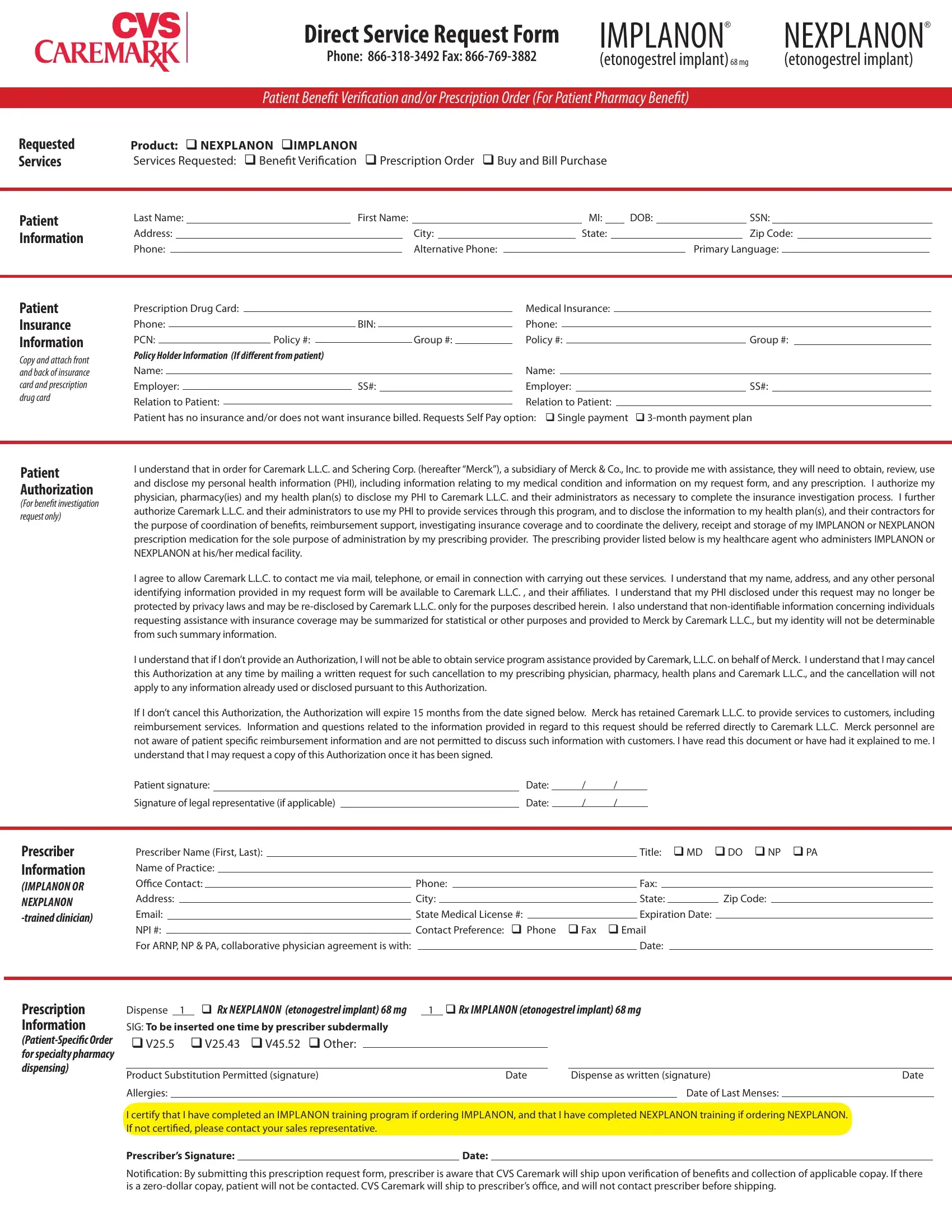
When it comes to managing reproductive health and family planning options, individuals often seek the most convenient and effective solutions. The Nexplanon CVS form serves a pivotal role in streamlining access to one such solution, providing a direct service request form for IMPLANON® and NEXPLANON® (etonogestrel implant)68 mg. This comprehensive form caters to patient benefit verification, prescription orders, and buy and bill purchases, ensuring that both patients and prescribers have a seamless process for obtaining these implants. With fields for patient information, insurance details, and prescriber credentials, the form facilitates a thorough scrutiny of benefits and covers all bases from prescription requests to delivery arrangements. Moreover, it underscores the importance of patient consent and authorization for using personal health information, a crucial step for privacy and transparency. The integration of insurance investigation, benefit coordination, and prescription medication delivery into one form reflects a tailored approach to healthcare provision, aiming to expedite and simplify the process for everyone involved.
| Question | Answer |
|---|---|
| Form Name | Nexplanon Cvs Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | merck nexplanon enrollment form 2021, nexplanon form, nexplanon application form 2021, nexplanon form 2021 |
Direct Service Request Form |
IMPLANON® |
NEXPLANON® |
Phone: |
(etonogestrel implant)68 mg |
(etonogestrel implant) |
Patient Beneit Veriication and/or Prescription Order (For Patient Pharmacy Beneit)
Requested |
Product: q NEXPLANON qIMPLANON |
Services |
Services Requested: q Beneit Veriication q Prescription Order q Buy and Bill Purchase |
|
|
Patient Information
Last Name: |
|
First Name: |
|
|
|
|
MI: |
|
|
DOB: |
|
|
|
SSN: |
|
|
|||||
Address: |
|
|
|
|
City: |
|
|
|
State: |
|
|
|
|
|
Zip Code: |
|
|
||||
Phone: |
|
|
|
|
|
Alternative Phone: |
|
|
|
|
|
|
|
Primary Language: |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Patient
Insurance
Information
Copy and attach front and back of insurance card and prescription drug card
Prescription Drug Card: |
|
|
|
|
|
|
|
|
|
|
Medical Insurance: |
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Phone: |
|
|
|
|
|
|
|
BIN: |
|
|
Phone: |
|
|
|
|
|
|
|
|
|
||||||
PCN: |
|
|
|
|
|
Policy #: |
|
|
|
|
Group #: |
|
|
Policy #: |
|
|
|
|
Group #: |
|||||||
Policy Holder Information (If diferent from patient) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
Name: |
|
|
|
|
|
|
|
|
|
|
|
|
Name: |
|
|
|
|
|
|
|||||||
Employer: |
|
|
|
|
|
|
SS#: |
|
|
Employer: |
|
|
SS#: |
|
||||||||||||
|
|
|
|
|
|
|
||||||||||||||||||||
Relation to Patient: |
|
|
|
|
|
|
|
|
|
|
|
Relation to Patient: |
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
Patient has no insurance and/or does not want insurance billed. Requests Self Pay option: q Single payment |
q |
|||||||||||||||||||||||||
Patient Authorization
(For beneit investigation request only)
I understand that in order for Caremark L.L.C. and Schering Corp. (hereafter “Merck”), a subsidiary of Merck & Co., Inc. to provide me with assistance, they will need to obtain, review, use and disclose my personal health information (PHI), including information relating to my medical condition and information on my request form, and any prescription. I authorize my physician, pharmacy(ies) and my health plan(s) to disclose my PHI to Caremark L.L.C. and their administrators as necessary to complete the insurance investigation process. I further authorize Caremark L.L.C. and their administrators to use my PHI to provide services through this program, and to disclose the information to my health plan(s), and their contractors for the purpose of coordination of beneits, reimbursement support, investigating insurance coverage and to coordinate the delivery, receipt and storage of my IMPLANON or NEXPLANON prescription medication for the sole purpose of administration by my prescribing provider. The prescribing provider listed below is my healthcare agent who administers IMPLANON or NEXPLANON at his/her medical facility.
I agree to allow Caremark L.L.C. to contact me via mail, telephone, or email in connection with carrying out these services. I understand that my name, address, and any other personal identifying information provided in my request form will be available to Caremark L.L.C. , and their ailiates. I understand that my PHI disclosed under this request may no longer be protected by privacy laws and may be
I understand that if I don’t provide an Authorization, I will not be able to obtain service program assistance provided by Caremark, L.L.C. on behalf of Merck. I understand that I may cancel this Authorization at any time by mailing a written request for such cancellation to my prescribing physician, pharmacy, health plans and Caremark L.L.C., and the cancellation will not apply to any information already used or disclosed pursuant to this Authorization.
If I don’t cancel this Authorization, the Authorization will expire 15 months from the date signed below. Merck has retained Caremark L.L.C. to provide services to customers, including reimbursement services. Information and questions related to the information provided in regard to this request should be referred directly to Caremark L.L.C. Merck personnel are not aware of patient speciic reimbursement information and are not permitted to discuss such information with customers. I have read this document or have had it explained to me. I understand that I may request a copy of this Authorization once it has been signed.
Patient signature: |
|
Date: |
/ |
/ |
|
Signature of legal representative (if applicable) |
|
Date: |
/ |
/ |
|
Prescriber Information
(IMPLANON OR
NEXPLANON
Prescriber Name (First, Last): |
|
|
|
|
|
|
|
Title: q MD |
q DO q NP q PA |
|||||||||
Name of Practice: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Oice Contact: |
|
Phone: |
|
|
Fax: |
|
|
|
|
|||||||||
Address: |
|
City: |
|
|
|
State: |
|
|
Zip Code: |
|
||||||||
Email: |
|
State Medical License #: |
|
|
Expiration Date: |
|
|
|
||||||||||
|
|
|
|
|
||||||||||||||
NPI #: |
|
Contact Preference: q Phone |
q Fax q Email |
|
|
|
||||||||||||
|
|
|
|
|||||||||||||||
For ARNP, NP & PA, collaborative physician agreement is with: |
|
|
|
|
|
|
Date: |
|
|
|
|
|||||||
Prescription |
Dispense 1 |
|
q Rx NEXPLANON (etonogestrel implant) 68 mg |
1 q Rx IMPLANON (etonogestrel implant) 68 mg |
|
|||||||||||
Information |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SIG: To be inserted one time by prescriber subdermally |
|
|
|
|
|
|
|
|
|
|||||||
qV25.5 |
qV25.43 qV45.52 q Other: |
|
|
|
|
|
|
|
|
|
|
|||||
for specialty pharmacy |
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
dispensing) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Product Substitution Permitted (signature) |
|
|
|
Date |
|
Dispense as written (signature) |
Date |
|||||||||
|
|
|
|
|
||||||||||||
|
Allergies: |
|
|
|
|
|
|
|
|
|
|
|
Date of Last Menses: |
|
|
|
|
I certify that I have completed an IMPLANON training program if ordering IMPLANON, and that I have completed NEXPLANON training if ordering NEXPLANON. |
|
||||||||||||||
|
If not certiied, please contact your sales representative. |
|
|
|
|
|
|
|
|
|
||||||
|
Prescriber’s Signature: |
|
|
|
Date: |
|
|
|
|
|
|
|||||
Notiication: By submitting this prescription request form, prescriber is aware that CVS Caremark will ship upon veriication of beneits and collection of applicable copay. If there is a
Prescriber Information
(IMPLANON OR NEXPLANON- trained clinician)
Buy and Bill Order Form |
IMPLANON® |
NEXPLANON® |
Phone: |
(etonogestrel implant)68 mg |
(etonogestrel implant) |
Purchase of IMPLANON and/or NEXPLANON (Buy and Bill)
Prescriber Name (First, Last): |
|
|
|
|
|
|
|
Title: q MD |
q DO q NP q PA |
|||||||||
Name of Practice: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Oice Contact: |
|
Phone: |
|
|
Fax: |
|
|
|
|
|||||||||
Address: |
|
City: |
|
|
State: |
|
|
Zip Code: |
|
|||||||||
Email: |
|
State Medical License #: |
|
|
Expiration Date: |
|
|
|
||||||||||
NPI #: |
|
Contact Preference: q Phone |
q Fax q Email |
|
|
|
||||||||||||
|
|
|
|
|||||||||||||||
For ARNP, NP & PA, collaborative physician agreement is with: |
|
|
|
|
|
|
Date: |
|
|
|
|
|||||||
Shipping Information
Ship to: q Prescriber’s Address Above |
q Address Below |
|
Requested Delivery Date: |
|
|
||||||||
Prescriber, Institution or Practice Name: |
|
|
|
|
|
|
|
|
|
|
|
||
Address: |
|
|
City: |
|
|
|
State: |
|
Zip Code: |
|
|||
Phone Number: |
|
|
|
|
|
Contact Name: |
|
|
|
||||
|
|
|
|
|
|
|
|||||||
CVS Caremark will invoice Purchaser at the time of each shipment. Payment to CVS Caremark for the products is due and payable within ninety (90) days after the date of CVS Caremark’s related invoice (“Payment Due Date”). Purchaser must sign a letter of agreement prior to irst shipment.
Bill to Address - Account Holder (If diferent than shipping information)
Buy & Bill
(Prescriber purchases, billed to the prescriber)
Physician, Institution or Practice Name: |
|
|
|
|
|
|
|
|
|
|
HIN: |
|
|
|
|
|
|
|
||||||||
Address: |
|
|
|
|
|
|
City: |
|
|
|
State: |
|
Zip Code: |
|
||||||||||||
Phone Number: |
|
|
|
|
|
|
Contact Name: |
|
|
|
|
|
|
|
|
|
|
|
||||||||
Quantity Requested: |
|
|
|
PRODUCT: IMPLANON |
NDC: |
|
||||||||||||||||||||
Quantity Requested: |
|
|
|
PRODUCT: NEXPLANON |
NDC: |
|
|
|
|
|
|
|
|
|
|
|||||||||||
Credit Card: Name on Card: |
|
|
|
|
|
|
|
|
Account #: |
|
|
|
|
|
|
|
Exp. Date: |
|
||||||||
Form of Business: q Hospital |
q Private Practice q PHS (340B) q Sub PHS (340B Prime Vendor) |
q FSS (DoD, VA, IHS) |
||||||||||||||||||||||||
|
|
q Planned Parenthood q Other (please specify): |
|
|
|
|
|
|
|
|
|
|
||||||||||||||
Tax Identiication Number: FEIN: |
|
|
|
|
|
|
SSN: |
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
Submit copy of tax exempt certiicate if eligible |
|
|
|
|
|
(IF FEIN NOT AVAILABLE) |
||||||||||||
Provider will be invoiced for all products [IMPLANON or NEXPLANON] purchased from Caremark, L.L.C. at the rates quoted at the
Signature: |
|
Print Name and Title: |
|
|
Date: |
|
If diferent from signature, provide the name of the IMPLANON and/or NEXPLANON trained clinician responsible for this order: |
|
|
|
|||
NOTE: To order NEXPLANON,
The information provided in response to your request for insurance coverage assistance will be based on statements of individuals not ailiated with Caremark, L.L.C or Schering Corporation (Merck), a subsidiary of Merck & Co., Inc. Neither Merck nor Caremark, L.L.C. make any warranties, expressed or implied, about the accuracy of this information. Insurance coverage status can change over time based on a variety of factors including, processing of additional claims that impact deductibles and/or coverage limits, changes in beneit design and a patient’s change in insurance carrier. The coverage information to be provided is intended for your reference only and does not guarantee current or future coverage for IMPLANON or
NEXPLANON.
Individual patient coverage reports will be made available to the extent that information is made available by the insurance plan. The goal is to respond to your request in one to two business days. This timing cannot be guaranteed based on the willingness of insurance companies to release insurance coverage information.
Fax to:
Important Instructions
When completing/submitting your
Direct Service Request Form
CVS Caremark can verify patient beneits on behalf of the prescriber. To expedite this process, please take a moment to read these instructions and complete each section of the form. You may also order at
1
2
3
4
1Patient Beneit Veriication
NOTE: Please notify your patients that CVS Caremark will attempt to reach them by phone to verify their acceptance of the product if there is a inancial responsibility due.
PATIENT INFORMATION: Please provide complete contact information for the patient.
PATIENT AUTHORIZATION: Please have patient read, sign and date.
PRESCRIBER: The prescriber listed on the form must be trained in the insertion and removal of IMPLANON if prescribing IMPLANON, or NEXPLANON, if prescribing NEXPLANON.
2Prescription Information
NOTE: To order IMPLANON and/or NEXPLANON by prescription for a participating patient, please complete the prescription section, in addition to patient information, patient insurance information, and prescriber information sections.
PRESCRIBER SIGNATURE: The individual signing this form must be the trained clinician who will be inserting IMPLANON and/or NEXPLANON.
NOTE: If your patient will be paying by cash, you may use this form as a prescription. Please check the box of either single payment or 3 month payment plan under the “Insurance Information”portion of this form.
Product will ship without patient contact if the patient has zero inancial responsibility.
3Shipping Information
NOTE: It is important that all shipping information be completed prior to submitting this form. If you have a requested delivery date, please indicate in the space provided.
4Buy and Bill Purchase
NOTE: To purchase IMPLANON and/or NEXPLANON for Buy and Bill, complete this section. This will allow IMPLANON Direct to ensure that IMPLANON and/or NEXPLANON is received on time. Purchaser must sign a letter of agreement with CVS Caremark prior to irst shipment.
SIGNATURE AUTHORIZATION: Buy and Bill purchases must be authorized by an individual with purchasing authority.
If this person is not trained on the product purchased, please identify the trained clinician responsible for the order.
Before submitting,
remember to....
qIndicate product requested
qIndicate services requested
qFill in the patient’s information, including Social Security Number; have patient sign
qMake sure the prescriber listed on the form is trained in inserting IMPLANON and/or
NEXPLANON
qAccurately and thoroughly complete the Insurance Information section, including all corresponding codes
qFax the completed form along with both sides of the patient’s insurance card
qTo contact IMPLANON Direct with any questions or concerns, please call
5
5Faxing the Form
Please fax the completed form, along with both sides of the patient’s insurance card and prescription drug card, to
IMPLANON and NEXPLANON are registered trademarks of N.V. Organon, a subsidiary of Merck & Co., Inc.
Copyright © 2011 Caremark, L.L.C.
IMPLANON®
(etonogestrel implant)68 mg
NEXPLANON®
(etonogestrel implant)