
universal health form nj 2021 can be completed in no time. Just use FormsPal PDF tool to finish the job right away. In order to make our tool better and easier to work with, we continuously develop new features, considering suggestions coming from our users. With just a few basic steps, you can start your PDF journey:
Step 1: Hit the orange "Get Form" button above. It'll open our tool so that you can begin filling out your form.
Step 2: The tool provides the capability to change PDF files in many different ways. Transform it by writing customized text, correct original content, and add a signature - all within the reach of a few mouse clicks!
It is an easy task to complete the form with our helpful tutorial! Here is what you want to do:
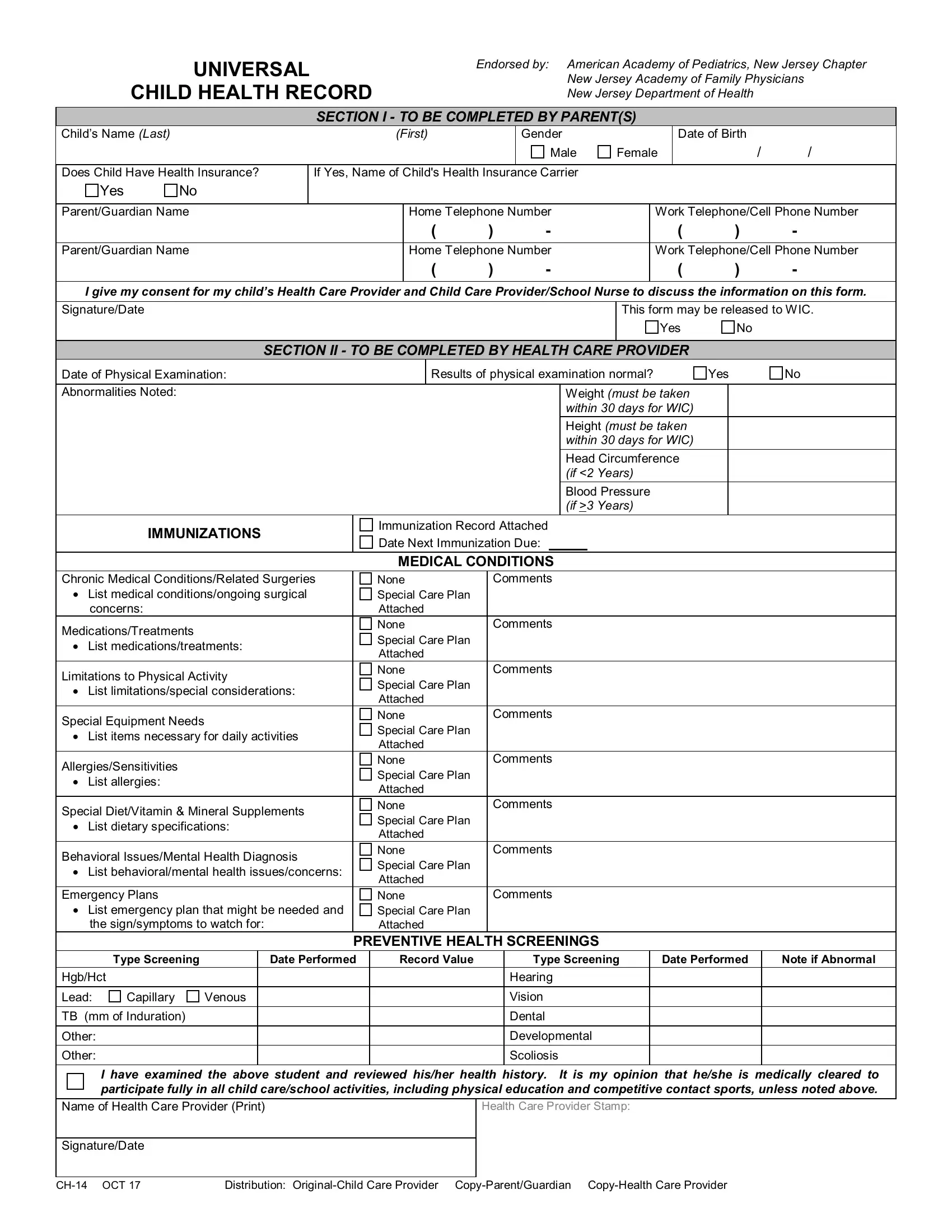
1. While submitting the universal health form nj 2021, make sure to include all important blank fields in its associated form section. This will help to speed up the process, which allows your information to be processed quickly and accurately.
2. Your next stage is to complete these fields: MEDICAL CONDITIONS Comments, concerns, MedicationsTreatments, List medicationstreatments, Limitations to Physical Activity, List limitationsspecial, Special Equipment Needs, List items necessary for daily, AllergiesSensitivities, List allergies, Special DietVitamin Mineral, List dietary specifications, Behavioral IssuesMental Health, List behavioralmental health, and Emergency Plans.
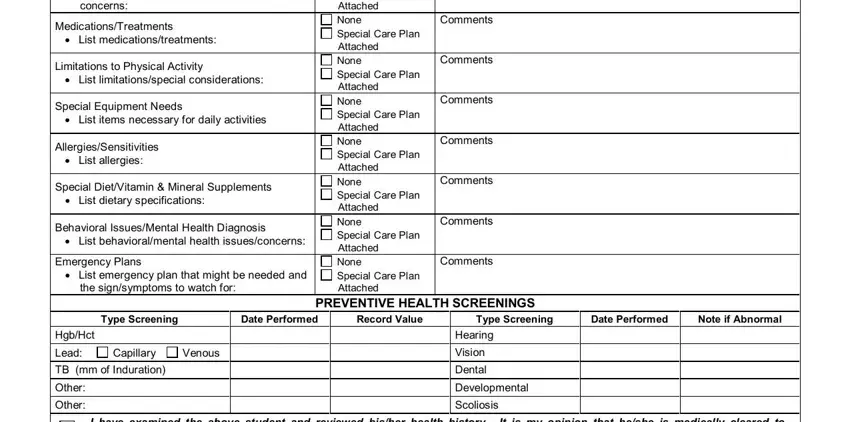
A lot of people frequently make some mistakes while completing Behavioral IssuesMental Health in this section. Ensure you review what you enter right here.
3. The next part is normally simple - fill out all the fields in Name of Health Care Provider Print, Health Care Provider Stamp, SignatureDate, CH OCT, and Distribution OriginalChild Care to complete the current step.

Step 3: Before moving on, check that blank fields were filled out as intended. Once you determine that it's correct, click “Done." After starting a7-day free trial account with us, you'll be able to download universal health form nj 2021 or send it via email promptly. The PDF will also be readily available via your personal account menu with your every edit. FormsPal is devoted to the confidentiality of our users; we make certain that all information entered into our tool continues to be protected.