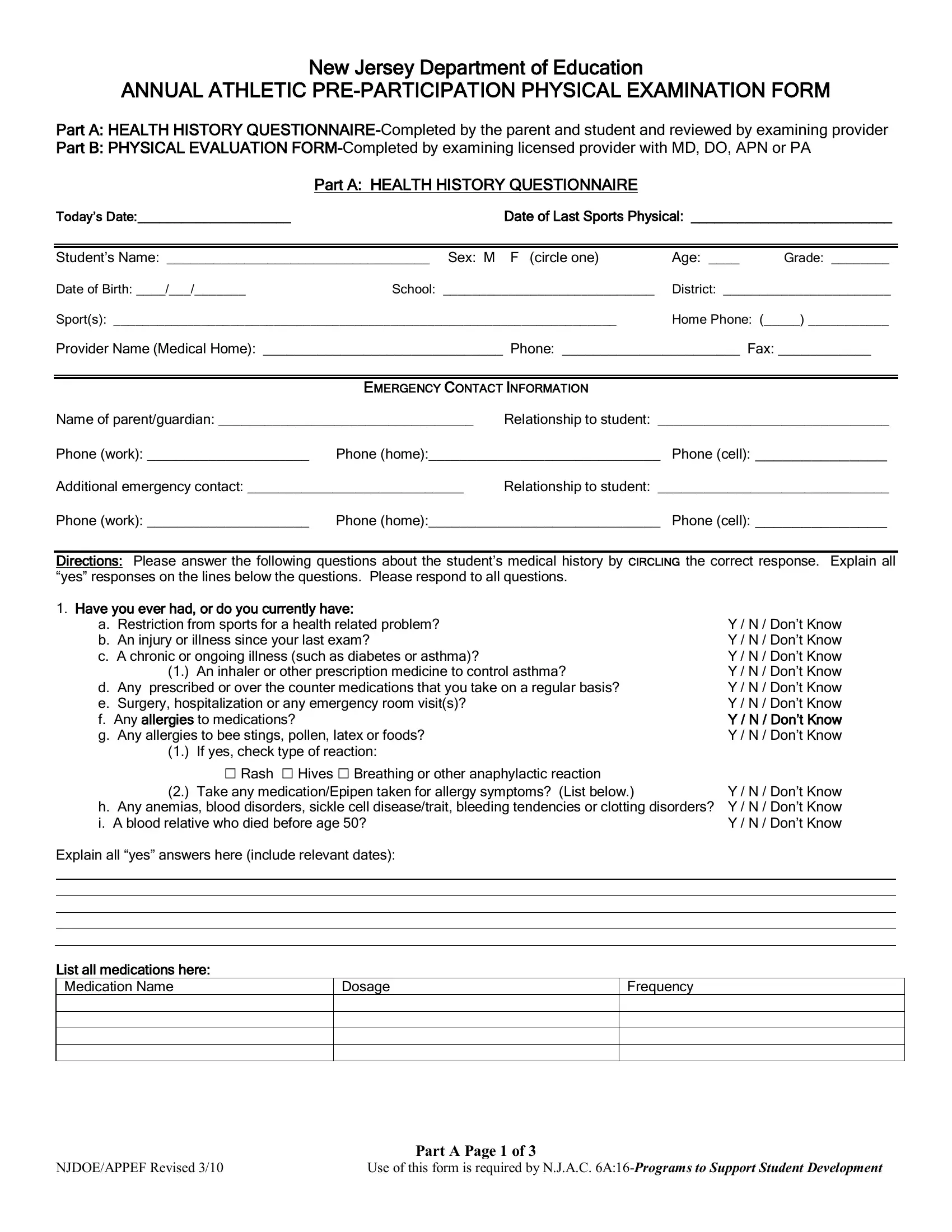
Embarking on a sports season in New Jersey schools requires meticulous preparation, not just in terms of physical training but also in ensuring the health and safety of students. This is where the New Jersey Department of Education's Annual Athletic Pre-Participation Physical Examination Form plays a crucial role. It's a comprehensive document designed to assess students' physical readiness for sports participation, safeguarding against potential risks associated with physical exertion. The form is divided into two essential parts - Part A: the Health History Questionnaire, which is to be completed by both the parent and the student and then reviewed by the examining provider, and Part B: the Physical Evaluation Form, which must be filled out by a licensed provider such as an MD, DO, APN, or PA. This critical document covers a broad array of health aspects from general information, emergency contacts, an in-depth medical history including questions on head and heart-related conditions, neuromuscular/orthopedic status, and even inquiries into psychological well-being, thereby ensuring a holistic assessment. Additionally, it addresses gender-specific health queries and requires a parent/guardian's signature to certify the accuracy of the provided information. In essence, this form acts as a preventive measure, aiming to ensure that all student-athletes are physically and medically fit to engage in athletic activities, thus fostering a safe environment for sporting excellence in New Jersey schools.
| Question | Answer |
|---|---|
| Form Name | Nj Sports Phisical Form |
| Form Length | 7 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 45 sec |
| Other names | new jersey school physical form, nj sports form, school physical form, sports physical form state of new jersey |

New Jersey Department of Education
ANNUAL ATHLETIC
Part A: HEALTH HISTORY
Part B: PHYSICAL EVALUATION
Part A: HEALTH HISTORY QUESTIONNAIRE
Today’s Date:_____________________ |
Date of Last Sports Physical: __________________________ |
||
|
|
|
|
|
|
|
|
Student’s Name: __________________________________ Sex: M F (circle one) |
Age: ____ |
Grade: ________ |
|
Date of Birth: ____/___/_______ |
School: _____________________________ |
District: _______________________ |
|
Sport(s): _____________________________________________________________________ |
Home Phone: (_____) ___________ |
||
Provider Name (Medical Home): _______________________________ Phone: _______________________ Fax: ____________
|
EMERGENCY CONTACT INFORMATION |
|
|
Name of parent/guardian: _________________________________ |
Relationship to student: ______________________________ |
||
Phone (work): _____________________ |
Phone (home):______________________________ |
Phone (cell): ______________ |
|
Additional emergency contact: ____________________________ |
Relationship to student: ______________________________ |
||
Phone (work): _____________________ |
Phone (home):______________________________ |
Phone (cell): ______________ |
|
Directions: Please answer the following questions about the student’s medical history by CIRCLING the correct response. Explain all “yes” responses on the lines below the questions. Please respond to all questions.
1.Have you ever had, or do you currently have:
a. Restriction from sports for a health related problem? |
Y / N / Don’t Know |
|
b. An injury or illness since your last exam? |
Y / N / Don’t Know |
|
c. A chronic or ongoing illness (such as diabetes or asthma)? |
Y / N / Don’t Know |
|
(1.) |
An inhaler or other prescription medicine to control asthma? |
Y / N / Don’t Know |
d. Any prescribed or over the counter medications that you take on a regular basis? |
Y / N / Don’t Know |
|
e. Surgery, hospitalization or any emergency room visit(s)? |
Y / N / Don’t Know |
|
f. Any allergies to medications? |
Y / N / Don’t Know |
|
g. Any allergies to bee stings, pollen, latex or foods? |
Y / N / Don’t Know |
|
(1.) |
If yes, check type of reaction: |
|
|
□ Rash □ Hives □ Breathing or other anaphylactic reaction |
|
(2.) |
Take any medication/Epipen taken for allergy symptoms? (List below.) |
Y / N / Don’t Know |
h. Any anemias, blood disorders, sickle cell disease/trait, bleeding tendencies or clotting disorders? Y / N / Don’t Know |
||
i. A blood relative who died before age 50? |
Y / N / Don’t Know |
|
Explain all “yes” answers here (include relevant dates):
List all medications here:
Medication Name |
Dosage |
Frequency |
|
|
|
|
|
|
|
|
|
|
|
|
Part A Page 1 of 3
NJDOE/APPEF Revised 3/10 |
Use of this form is required by N.J.A.C. |
2.Have you ever had, or do you currently have, any of the following
a. Concussion or head injury (including “bell rung” or a “ding”)? |
Y / N / Don’t Know |
b. Memory loss? |
Y / N / Don’t Know |
c. Knocked out? |
Y / N / Don’t Know |
c. A seizure? |
Y / N / Don’t Know |
d. Frequent or severe headaches (With or without exercise)? |
Y / N / Don’t Know |
e. Fuzzy or blurry vision |
Y / N / Don’t Know |
f. Sensitivity to light/noise |
Y / N / Don’t Know |
Explain all “yes” answers here (include relevant dates):
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
3.Have you ever had, or do you currently have, any of the following
a. Restriction from sports for heart problems? |
Y / N / Don’t Know |
|
b. Chest pain or discomfort? |
Y / N / Don’t Know |
|
c. |
Heart murmur? |
Y / N / Don’t Know |
d. |
High blood pressure? |
Y / N / Don’t Know |
e. |
Elevated cholesterol level? |
Y / N / Don’t Know |
f. |
Heart infection? |
Y / N / Don’t Know |
g. |
Dizziness or passing out during or after exercise without known cause? |
Y / N / Don’t Know |
h.Has a provider ever ordered a heart test ( EKG, echocardiogram, stress test, Holter monitor)? Y / N / Don’t Know
i. |
Racing or skipped heartbeats? |
Y / N / Don’t Know |
j. |
Unexplained difficulty breathing or fatigue during exercise? |
Y / N / Don’t Know |
k.Any family member (blood relative):
(1.) |
Under age 50 with a heart condition? |
Y / N / Don’t Know |
(2.) |
With Marfan Syndrome? |
Y / N / Don’t Know |
(3.) |
Died of a heart problem before age 50? If yes, at what age? _____________________ |
Y / N / Don’t Know |
(4.) |
Died with no known reason? |
Y / N / Don’t Know |
(5.) |
Died while exercising? If yes, was it during or after? (Circle one.) |
Y / N / Don’t Know |
Explain all “yes” answers here (include relevant dates):
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
4.Have you ever had, or do you currently have, any of the following eye, ear, nose, mouth or throat conditions:
a. Vision problems? |
Y / N / Don’t Know |
(1.) Wear contacts, eyeglasses or protective eye wear? (Circle which type.) |
Y / N / Don’t Know |
b. Hearing loss or problems? |
Y / N / Don’t Know |
(1.) Wear hearing aides or implants? |
Y / N / Don’t Know |
c. Nasal fractures or frequent nose bleeds? |
Y / N / Don’t Know |
d. Wear braces, retainer or protective mouth gear? |
Y / N / Don’t Know |
e. Frequent strep or any other conditions of the throat (e.g. tonsillitis)? |
Y / N / Don’t Know |
Explain all “yes” answers here (include relevant dates):
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
5.Have you ever had, or do you currently have, any of the following neuromuscular/orthopedic conditions:
a. Numbness, a “burner”, “stinger” or pinched nerve? |
Y / N / Don’t Know |
|
b. |
A sprain? |
Y / N / Don’t Know |
c. |
A strain? |
Y / N / Don’t Know |
d. |
Swelling or pain in muscles, tendons, bones or joints? |
Y / N / Don’t Know |
e. |
Dislocated joint(s)? |
Y / N / Don’t Know |
f. |
Upper or lower back pain? |
Y / N / Don’t Know |
g. |
Fracture(s), stress fracture(s), or broken bone(s)? |
Y / N / Don’t Know |
h. |
Do you wear any protective braces or equipment? |
Y / N / Don’t Know |
Explain all (yes) answers here (include relevant dates):
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
Part A Page 2 of 3
NJDOE/APPEF Revised 3/10 |
Use of this form is required by N.J.A.C. |

6.Have you ever had or do you currently have any of the following general or exercise related conditions: a. Difficulty breathing?
(1.) |
During exercise? |
Y / N / Don’t Know |
(2.) |
After running one mile? |
Y / N / Don’t Know |
(3.) |
Coughing, wheezing or shortness of breath in weather changes? |
Y / N / Don’t Know |
(4.) |
Y / N / Don’t Know |
|
|
i. Controlled with medication? (specify __________________________) |
Y / N / Don’t Know |
|
ii. Experience dizziness, passing out or fainting? |
Y / N / Don’t Know |
b. Viral infections (e.g. mono, hepatitis, coxsackie virus)? |
Y / N / Don’t Know |
|
c. Become tired more quickly than others? |
Y / N / Don’t Know |
|
d. Any of the following skin conditions: |
|
|
(1.) |
Cold sores/herpes, impetigo, MRSA, ringworm, warts? |
Y / N / Don’t Know |
(2.) |
Sun sensitivity? |
Y / N / Don’t Know |
e. Weight gain/loss (of 10 pounds or more)? |
Y / N / Don’t Know |
|
(1.) |
Do you want to weigh more or less than you do now? |
Y / N / Don’t Know |
f. Ever had feelings of depression? |
Y / N / Don’t Know |
|
g. |
Y / N / Don’t Know |
|
(1.) |
Heat exhaustion (cool, clammy, damp skin)? |
Y / N / Don’t Know |
(2.) |
Heat stroke (hot, red, dry skin)? |
Y / N / Don’t Know |
(3.) |
Muscle cramps? |
Y / N / Don’t Know |
h. Absence or loss of an organ (e.g. kidney, eyeball, spleen, testicle, ovary)? |
Y / N / Don’t Know |
|
Explain all “yes” answers here (include relevant dates):
__________________________________________________________________________________________________________________________
__________________________________________________________________________________________________________________________
_________________________________________________________________________________________________________________________
7. |
Females only: |
|
|
|
|
Age of onset of menstruation:______ |
How many menstrual periods in the last twelve (12) months? |
________ |
|
|
|
How many periods missed in the last twelve (12) months? |
________ |
|
8. |
Males only: |
|
|
|
|
Have you had any swelling or pain in your testicles or groin? |
Y / N / Don’t Know |
||
PARENT/GUARDIAN SIGNATURE
I certify that the information provided herein is accurate to the best of my knowledge as of the date of my signature.
_______________________________________ |
_________________ |
Signature, Parent/Guardian or Student Age 18 |
Date of Signature: |
THIS COMPLETED AND SIGNED HEALTH HISTORY MUST BE REVIEWED BY THE
EXAMINING PROVIDER AT THE TIME OF THE MEDICAL EXAM.
Part A Page 3 of 3
NJDOE/APPEF Revised 3/10 |
Use of this form is required by N.J.A.C. |

ANNUAL ATHLETIC
Part B: Physical Evaluation Form
(Completed by the examining licensed provider MD, DO, APN or PA)
Student’s Name: __________________________________ Sport(s): _____________________________________________________
Sex: M F (circle one) Age: ________ Grade: _____________ |
Date of Birth: _________________________________________ |
Address: ___________________________________________________________________________________________________________
City/State/Zip:________________________________________________ |
Home Phone: _________________________________________ |
School: _____________________________________________________ |
District: _____________________________________________ |
Parent/Guardian’s Full Name: __________________________________________________________________________________________
- EXAMINING PHYSICIAN/PROVIDER CONTACT INFORMATION-
|
If conducted by school physician check here □ |
|
|
|
|
|||
|
Name: _______________________________ |
Phone: __________________________ |
Fax: _________________ |
|||||
|
Address:______________________________ |
City/State/Zip:_____________________________________________ |
||||||
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
||
|
|
|
- FINDINGS OF PHYSICAL EVALUATION - |
|
|
|||
|
Height: _________ |
Weight: _________ |
Blood Pressure: ______/_______ Pulse: _____bpm. |
|||||
|
Vision: R 20/____ L 20/ ____ |
Corrected: Y / N |
Contacts: Y / N |
Glasses: Y / N |
|
|||
|
|
|
|
|
|
|||
|
INDICATORS |
|
NORMAL? |
|
ABNORMAL FINDINGS/COMMENTS |
|||
|
|
|
|
|
|
|
|
|
|
General Appearance |
|
YES |
|
|
|
|
|
|
Head/Neck |
|
YES |
|
|
|
|
|
|
Eyes/Sclera/Pupils |
|
YES |
|
|
|
|
|
|
Ears |
|
YES |
|
|
|
|
|
|
Gross Hearing |
|
YES |
|
|
|
|
|
|
Nose/Mouth/Throat |
|
YES |
|
|
|
|
|
|
Lymph Glands |
|
YES |
|
|
|
|
|
|
Cardiovascular |
|
YES |
|
|
|
|
|
|
Heart Rate |
|
YES |
|
|
|
|
|
|
Rhythm |
|
YES |
|
|
|
|
|
|
Murmur |
|
ABSENT |
|
|
|
|
|
|
If murmur present |
|
|
|
Standing makes it: |
Louder |
Softer |
No Change |
|
|
|
|
|
Squatting makes it: |
Louder |
Softer |
No Change |
|
|
|
|
|
Valsalva makes it: |
Louder |
Softer |
No Change |
|
Femoral Pulses |
|
YES |
|
|
|
|
|
|
Lungs: Auscultation/Percussion |
|
YES |
|
|
|
|
|
|
Chest Contour |
|
YES |
|
|
|
|
|
|
Skin |
|
YES |
|
|
|
|
|
|
Abdomen (liver, spleen, masses) |
|
YES |
|
|
|
|
|
|
Assessment of physical maturation or |
YES |
|
|
|
|
|
|
|
Tanner Scale |
|
|
|
|
|
|
|
|
Testicular Exam (Males Only) |
|
YES |
|
|
|
|
|
|
Neck/Back/Spine: |
|
YES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Range of Motion |
|
YES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Scoliosis |
|
ABSENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Upper Extremities: (ROM, Strength, |
YES |
|
|
|
|
|
|
|
Stability) |
|
|
|
|
|
|
|
|
Lower Extremities: (ROM, Strength, |
YES |
|
|
|
|
|
|
|
Stability) |
|
|
|
|
|
|
|
|
Neurological: Balance & Coordination |
YES |
|
|
|
|
|
|
|
Hernia |
|
ABSENT |
|
|
|
|
|
|
Evidence of Marfan Syndrome |
|
ABSENT |
|
|
|
|
|
|
|
|
Part B Page 1 of 4 |
|
|
|
||
|
NJDOE/APPEF Revised 3/10 |
|
Use of this form is required by N.J.A.C. |
|||||

Most recent immunizations and dates administered:
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
Medications currently prescribed, with dose and frequency:
Medication Name
Dosage
Frequency
Additional observations:
________________________________________________________________________________________________________________________
________________________________________________________________________________________________________________________
________________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
General Diagnosis: ____________________________________________________________________________________________
____________________________________________________________________________________________________________
___________________________________________________________________________________________________________
General Recommendations:
____________________________________________________________________________________________________________
___________________________________________________________________________________________________________
THE HISTORY PREPARED BY THE PARENT/STUDENT MUST BE REVIEWED BY THE EXAMINING PROVIDER AT THE TIME OF THE PHYSICAL EXAMINATION.
Part B Page 2 of 4
NJDOE/APPEF Revised 3/10 |
Use of this form is required by N.J.A.C. |
CLEARANCES: This section is completed by the examining healthcare provider.
After examining the student and reviewing the medical history the student is:
A.Cleared for participation in all sports without restrictions.
B.Not cleared for participation in any sport until evaluation/treatment of:
___________________________________________________________________________________
C.Cleared for limited participation in the following types of sports only. Please see below for sport classifications. CHECK ALL THAT APPLY
___ |
CONTACT/COLLISION |
___ |
|
___ |
LIMITED CONTACT |
___ |
Limitations due to: ___________________________________________________________________
________________________________________________
NOTES TO THE EXAMINING PROVIDER
Conditions requiring clearance before sports participation include, but are not limited to the following:
Anaphylaxis; Atlantoaxial instability; Bleeding disorder; Hypertension; Congenital heart disease; Dysrhythmia; Mitral valve prolapse; Heart murmur; Cerebral palsy; Diabetes mellitus; Eating disorders; Heat illness history;
SAMPLES OF CLASSIFICATION OF SPORTS BY CONTACT
Contact/Collision |
|
Limited Contact |
|
||
|
|
|
Strenuous |
|
|
Basketball |
|
Baseball |
Discus |
|
Bowling |
Diving |
|
Cheerleading |
Javelin |
|
Golf |
Field Hockey |
|
Fencing |
Shot put |
|
|
Football |
|
High Jump |
Rowing |
|
|
Ice Hockey |
|
Pole vault |
Running/Cross Country |
|
|
Lacrosse |
|
Gymnastics |
Strength Training |
|
|
Soccer |
|
Skiing |
Swimming |
|
|
Wrestling |
|
Softball |
Tennis |
|
|
|
|
Volleyball |
Track |
|
|
Effects of physiologic maneuvers on heart sounds |
Physical Stigmata of Marfan’s Syndrome |
||
Standing |
Increases murmur of HCM |
Kyphosis |
|
|
|
Decreases murmur of AS, MR |
High arched palate |
|
|
MVP click occurs earlier in systole |
Pectus excavatum |
|
|
|
Arachnodactyly |
Squatting |
Increases murmur of AS, MR, AI |
Arm span > height 1.05:1 or greater |
|
|
|
Decreases murmur of MCH |
Mitral Valve Prolapse |
|
|
MVP click delayed |
Aortic Insufficiency |
|
|
|
Myopia |
Valsalva |
Increases murmur of HCM |
Lenticular dislocation |
|
|
|
Decreases murmur of AS, MR |
|
|
|
MVP click occurs earlier in systole |
|
HCM: |
Hypertrophic Cardio Myopathy |
|
|
AS: |
Aortic Stenosis |
|
|
AI: |
Aortic Insufficiency |
|
|
MR: |
Mitral Regugitation |
|
|
MVP: |
Mitral Valve Prolapse |
|
|
|
Part B Page 3 of 4 |
NJDOE/APPEF Revised 3/10 |
Use of this form is required by N.J.A.C. |
HISTORY REVIEWED AND STUDENT EXAMINED BY: |
Physician’s/Provider’s Stamp: |
Primary Care Provider
School Physician Provider
License Type:
MD/DO
APN
PA
PHYSICIAN’S/PROVIDER’S SIGNATURE: __________________________________________________
Today’s Date: ______________ |
Date of Exam: ______________ |
RESERVED FOR SCHOOL DISTRICT USE
NOTE: N.J.A.C.
History and Physical Reviewed By: |
__________________________________ |
Date: _______________ |
||
Title of Reviewer (please check one): |
School Nurse |
School Physician |
||
Medical Eligibility Notification Sent to Parent/Guardian by School Physician |
______________________ |
|||
Date
Letter of notification is attached.
OR
Parent notification indicates that:
Participation Approved without limitations.
Participation Approved with limitations pending evaluation.
Participation NOT Approved
Reason(s) for Disapproval: ____________________________________________________________
_____________________________________________________________________________________
Part B Page 4 of 4
NJDOE/APPEF Revised 3/10 |
Use of this form is required by N.J.A.C. |