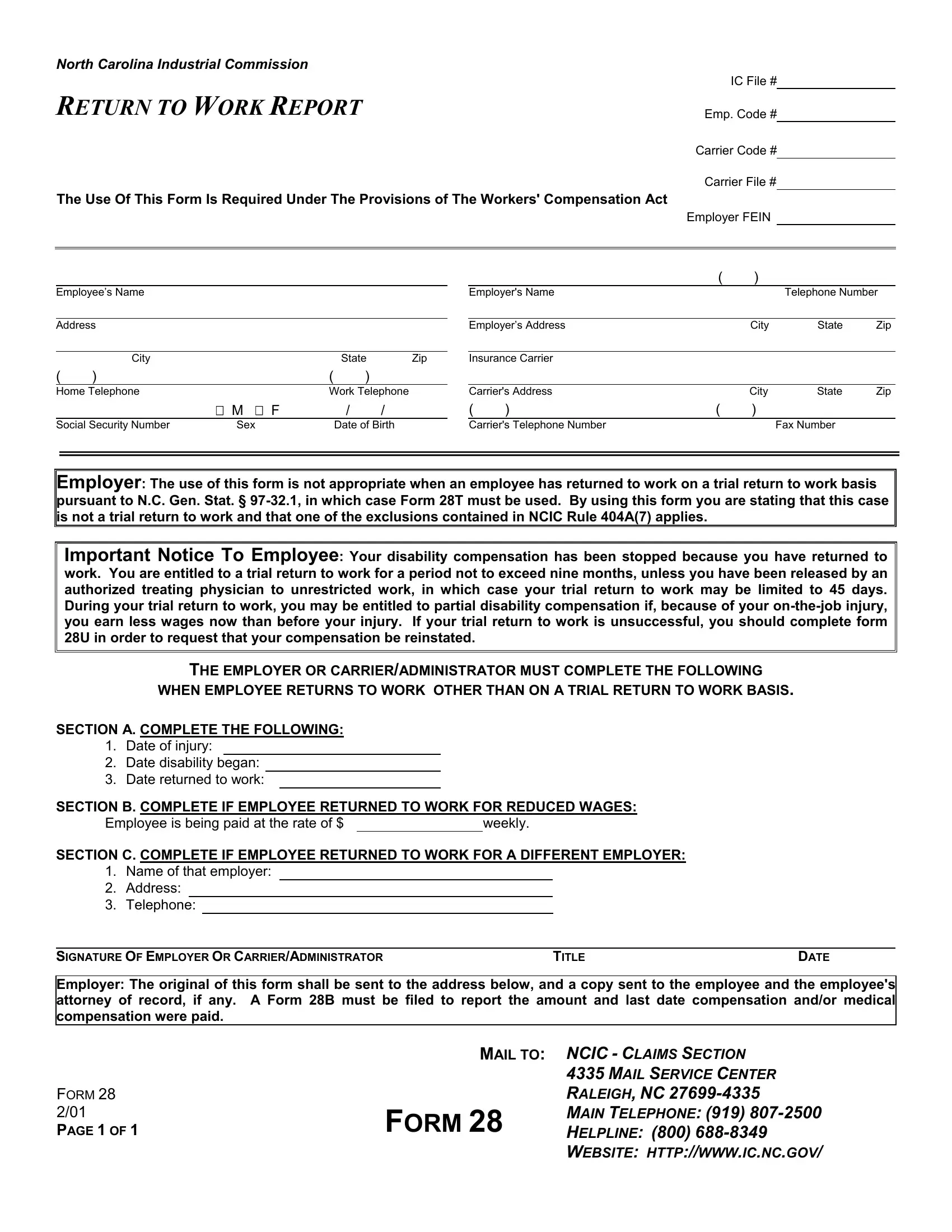
When an individual in North Carolina returns to work after being out due to a workplace injury, the North Carolina Industrial Commission's Form 28, titled "Return to Work Report," plays a crucial role. This document is an essential piece of the puzzle in the state's workers' compensation process, complying with the Workers' Compensation Act. It's designed to communicate the change in employment status of an injured worker, whether they're returning at full capacity, with restrictions, or at reduced wages. A critical feature of Form 28 is its clear distinction from Form 28T, which is used for trial returns to work as per N.C. Gen. Stat. § 97-32.1. It meticulously outlines the need for employers to report a non-trial return to work and specifies the conditions under which disability compensation is ceased, highlighting the potential eligibility for partial disability compensation during a trial return that doesn't exceed nine months. Furthermore, it provides instructions for workers whose trial return to work is unsuccessful on how to request the reinstatement of their compensation. This form serves not just as a bureaucratic requirement but as a safeguard for the rights of workers, ensuring they have the necessary information and processes to navigate their return to employment following an injury, and it encapsulates the attention to detail and worker-focused approach of North Carolina's system.
| Question | Answer |
|---|---|
| Form Name | North Carolina Form 28 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | HTTP, 404A, FEIN, North_Carolina |
NORTH CAROLINA INDUSTRIAL COMMISSION
IC File #
RETURN TO WORK REPORT
Emp. Code #
Carrier Code # Carrier File #
The Use Of This Form Is Required Under The Provisions of The Workers' Compensation Act
Employer FEIN
Employee’s Name
Address
|
City |
|
|
State |
Zip |
( |
) |
|
( |
) |
|
Home Telephone |
|
Work Telephone |
|||
|
|
M F |
|
/ |
/ |
Social Security Number |
Sex |
|
Date of Birth |
||
|
|
( |
) |
|
|
Employer's Name |
|
|
Telephone Number |
||
|
|
|
|
|
|
Employer’s Address |
|
City |
State |
Zip |
|
|
|
|
|
|
|
Insurance Carrier |
|
|
|
|
|
|
|
|
|
|
|
Carrier's Address |
|
City |
State |
Zip |
|
( |
) |
( |
) |
|
|
Carrier's Telephone Number |
|
|
Fax Number |
|
|
Employer: The use of this form is not appropriate when an employee has returned to work on a trial return to work basis pursuant to N.C. Gen. Stat. §
Important Notice To Employee: Your disability compensation has been stopped because you have returned to work. You are entitled to a trial return to work for a period not to exceed nine months, unless you have been released by an authorized treating physician to unrestricted work, in which case your trial return to work may be limited to 45 days. During your trial return to work, you may be entitled to partial disability compensation if, because of your
THE EMPLOYER OR CARRIER/ADMINISTRATOR MUST COMPLETE THE FOLLOWING
WHEN EMPLOYEE RETURNS TO WORK OTHER THAN ON A TRIAL RETURN TO WORK BASIS.
SECTION A. COMPLETE THE FOLLOWING:
1.Date of injury:
2.Date disability began:
3.Date returned to work:
SECTION B. COMPLETE IF EMPLOYEE RETURNED TO WORK FOR REDUCED WAGES:
Employee is being paid at the rate of $ |
|
weekly. |
SECTION C. COMPLETE IF EMPLOYEE RETURNED TO WORK FOR A DIFFERENT EMPLOYER:
1.Name of that employer:
2.Address:
3.Telephone:
SIGNATURE OF EMPLOYER OR CARRIER/ADMINISTRATOR |
TITLE |
DATE |
Employer: The original of this form shall be sent to the address below, and a copy sent to the employee and the employee's attorney of record, if any. A Form 28B must be filed to report the amount and last date compensation and/or medical compensation were paid.
|
MAIL TO: NCIC - CLAIMS SECTION |
|
|
|
4335 MAIL SERVICE CENTER |
FORM 28 |
|
RALEIGH, NC |
2/01 |
FORM 28 |
MAIN TELEPHONE: (919) |
PAGE 1 OF 1 |
HELPLINE: (800) |
|
WEBSITE: HTTP://WWW.IC.NC.GOV/