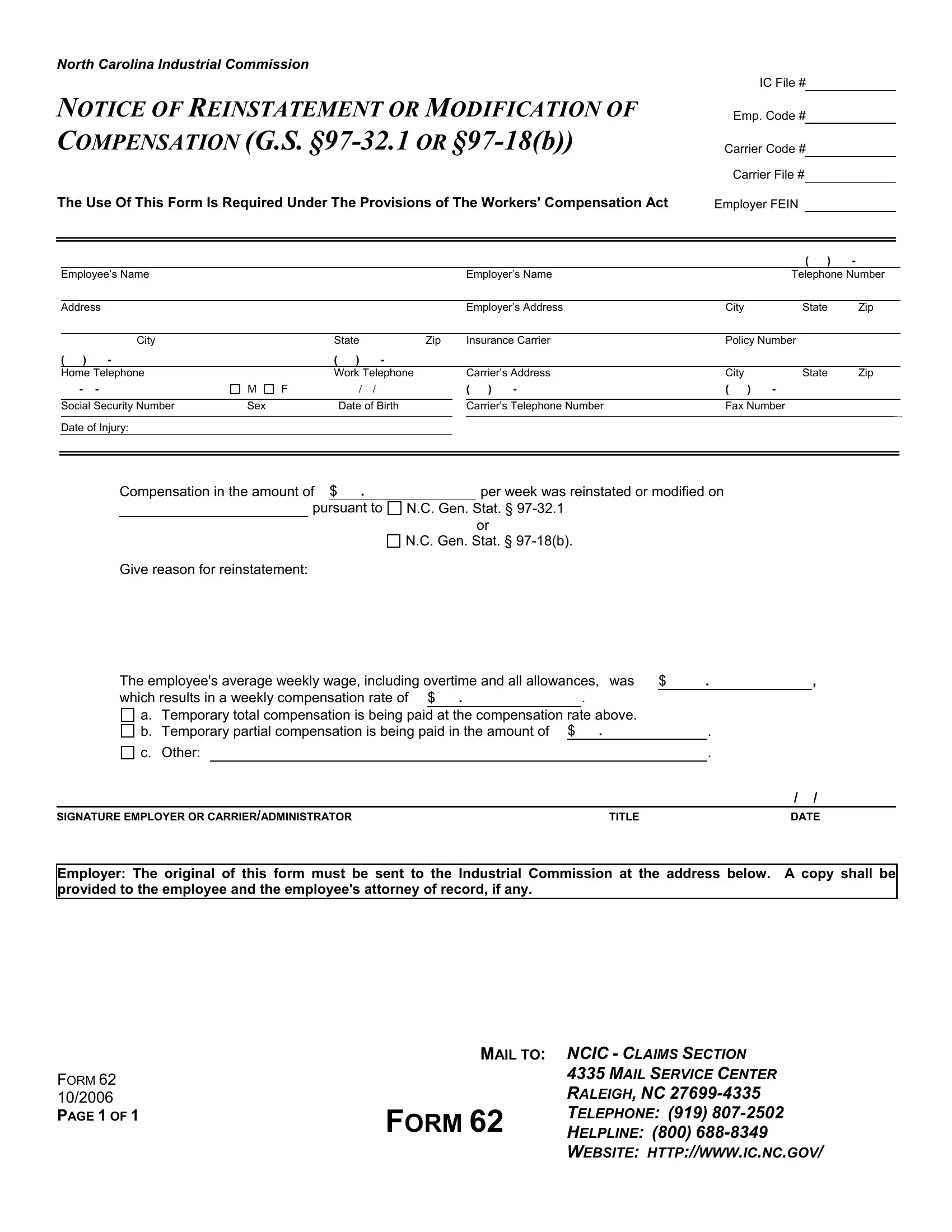
For many navigating through the complexities of workers' compensation claims within North Carolina, understanding the specifics of required documentation is crucial. One such document, the North Carolina 62 form, acts as a pivotal communication tool in the process of reinstating or modifying compensation under the Workers' Compensation Act. Mandated by the provisions of G.S. §97-32.1 or §97-18(b), this form is essential for informing the North Carolina Industrial Commission about changes in a workers' compensation claim. It meticulously records details such as the employer’s and employee's names, addresses, and contact information, alongside the specific nature of the compensation amendment - whether it's a reinstatement or modification. Furthermore, it requires disclosure of the employee’s compensation rate, based on their average weekly wage, which may include overtime and allowances, establishing the new basis for either temporary total or partial compensation payments. Understanding the function and proper use of this form not only aids in ensuring compliance with state laws but also facilitates the smoother administration of workers' compensation benefits, making it an indispensable document for both employers and employees alike in maintaining clarity and transparency throughout the claims process.
| Question | Answer |
|---|---|
| Form Name | North Carolina Form 62 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | NC, North_Carolina, REINSTATEMENT, pursuant |
NORTH CAROLINA INDUSTRIAL COMMISSION
IC File #
NOTICE OF REINSTATEMENT OR MODIFICATION OF
COMPENSATION (G.S.
Emp. Code #
Carrier Code # Carrier File #
The Use Of This Form Is Required Under The Provisions of The Workers' Compensation Act |
Employer FEIN |
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
( ) |
- |
|
|
|
Employee’s Name |
|
|
|
|
|
|
Employer’s Name |
|
Telephone Number |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Address |
|
|
|
|
|
|
Employer’s Address |
City |
State |
Zip |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
City |
|
State |
|
Zip |
|
Insurance Carrier |
Policy Number |
|
|
|||
( ) |
- |
|
( |
) |
- |
|
|
|
|
|
|
|
|
|
|
Home Telephone |
|
Work Telephone |
|
|
Carrier’s Address |
City |
State |
Zip |
|
||||
- |
- |
M |
F |
/ |
/ |
|
( ) - |
( ) |
- |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||||
|
Social Security Number |
Sex |
|
Date of Birth |
|
|
Carrier’s Telephone Number |
Fax Number |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of Injury:
Compensation in the amount of $ . |
|
per week was reinstated or modified on |
|
|
|
|
|
pursuant to |
N.C. Gen. Stat. § |
||
or
N.C. Gen. Stat. §
Give reason for reinstatement:
The employee's average weekly wage, including overtime and all allowances, was |
$ |
. |
, |
||||||
which results in a weekly compensation rate of $ |
. |
|
. |
|
|
|
|
||
|
|
|
|
|
|
|
|
||
a. Temporary total compensation is being paid at the compensation rate above. |
|
|
|
|
|||||
b. Temporary partial compensation is being paid in the amount of |
$ |
. |
|
|
. |
|
|||
c. Other: |
|
|
|
|
|
|
. |
|
|
|
|
|
|
|
|
|
/ |
/ |
|
SIGNATURE EMPLOYER OR CARRIER/ADMINISTRATOR |
|
|
TITLE |
|
|
DATE |
|||
Employer: The original of this form must be sent to the Industrial Commission at the address below. A copy shall be provided to the employee and the employee's attorney of record, if any.
|
MAIL TO: NCIC - CLAIMS SECTION |
|
FORM 62 |
|
4335 MAIL SERVICE CENTER |
|
RALEIGH, NC |
|
10/2006 |
|
|
PAGE 1 OF 1 |
FORM 62 |
TELEPHONE: (919) |
|
HELPLINE: (800) |
|
WEBSITE: HTTP://WWW.IC.NC.GOV/