Are you a North Carolina resident looking to file an estate tax return? If so, the NC-60 Form is likely your first step. This document outlines important information relating to the estate of a decedent (the deceased) in order to properly calculate and pay taxes due. In this blog post, we will cover everything you need to know about filing your NC-60 form, including how and when it must be filed, what type of information is collected on it, as well as any additional resources that may prove useful in its completion. Let's get started!
| Question | Answer |
|---|---|
| Form Name | North Carolina Form 60 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | compensable, particularity, RALEIGH, HTTP |

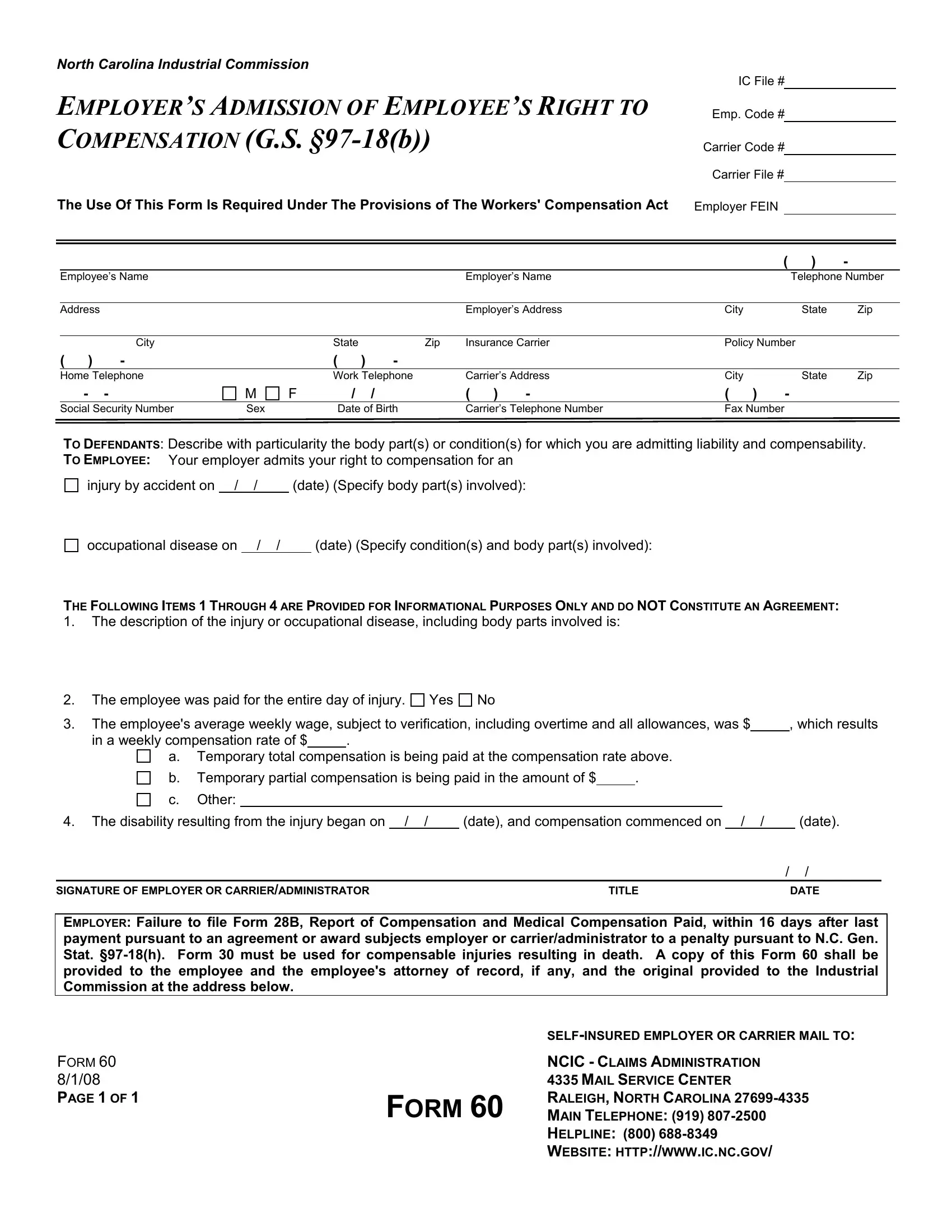
NORTH CAROLINA INDUSTRIAL COMMISSION
IC File #
EMPLOYER’S ADMISSION OF EMPLOYEE’S RIGHT TO
COMPENSATION (G.S.
Emp. Code #
Carrier Code # Carrier File #
The Use Of This Form Is Required Under The Provisions of The Workers' Compensation Act |
Employer FEIN |
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
( |
) |
- |
|
|
|
Employee’s Name |
|
|
|
|
|
Employer’s Name |
|
|
|
Telephone Number |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|
Employer’s Address |
City |
|
|
State |
Zip |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
City |
|
State |
|
Zip |
Insurance Carrier |
Policy Number |
|
|
|||||
( ) |
- |
|
( |
) |
- |
|
|
|
|
|
|
|
|
|
|
|
Home Telephone |
|
Work Telephone |
|
Carrier’s Address |
City |
|
|
State |
Zip |
|
||||
- |
- |
M |
F |
/ |
/ |
|
( ) |
- |
( ) |
- |
|
|
|
||
|
Social Security Number |
Sex |
|
Date of Birth |
|
Carrier’s Telephone Number |
Fax Number |
|
|
|
|||||
TO DEFENDANTS: Describe with particularity the body part(s) or condition(s) for which you are admitting liability and compensability.
TO EMPLOYEE: Your employer admits your right to compensation for an
injury by accident on / |
/ |
(date) (Specify body part(s) involved): |
||
|
|
|
|
|
occupational disease on |
/ / |
|
(date) (Specify condition(s) and body part(s) involved): |
|
THE FOLLOWING ITEMS 1 THROUGH 4 ARE PROVIDED FOR INFORMATIONAL PURPOSES ONLY AND DO NOT CONSTITUTE AN AGREEMENT:
1.The description of the injury or occupational disease, including body parts involved is:
2.The employee was paid for the entire day of injury.
Yes
No
3. |
The employee's average weekly wage, subject to verification, including overtime and all allowances, was $ |
, which results |
||||||||||||
|
in a weekly compensation rate of $ |
|
. |
|
|
|
|
|
|
|
|
|
|
|
|
a. Temporary total compensation is being paid at the compensation rate above. |
|
|
|||||||||||
|
b. Temporary partial compensation is being paid in the amount of $ |
. |
|
|
|
|
|
|||||||
|
c. Other: |
|
|
|
|
|
|
|
|
|
|
|
|
|
4. |
The disability resulting from the injury began on / / |
(date), and compensation commenced on / / |
|
(date). |
||||||||||
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|||
SIGNATURE OF EMPLOYER OR CARRIER/ADMINISTRATOR |
|
|
TITLE |
DATE |
||||||||||
EMPLOYER: Failure to file Form 28B, Report of Compensation and Medical Compensation Paid, within 16 days after last payment pursuant to an agreement or award subjects employer or carrier/administrator to a penalty pursuant to N.C. Gen. Stat.
|
|
|
FORM 60 |
|
NCIC - CLAIMS ADMINISTRATION |
8/1/08 |
|
4335 MAIL SERVICE CENTER |
PAGE 1 OF 1 |
FORM 60 |
RALEIGH, NORTH CAROLINA |
|
MAIN TELEPHONE: (919) |
|
|
|
HELPLINE: (800) |
|
|
WEBSITE: HTTP://WWW.IC.NC.GOV/ |