Are you looking to file a North Carolina Franchise Tax Return? The Form 62 may be the key document for your filing needs. The Department of Revenue in North Carolina requires businesses registered within the state to complete this form each year, and it's important to make sure everything is correctly filled out for submission. In this blog post, we'll discuss all aspects of Form 62 including who must file it, when it's due, and how to prepare one properly so that you can avoid any potential problems with the State of North Carolina. By the end of this article you should have a clearer understanding on all components related to Form 62.
| Question | Answer |
|---|---|
| Form Name | North Carolina Form 62 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | NC, North_Carolina, REINSTATEMENT, pursuant |
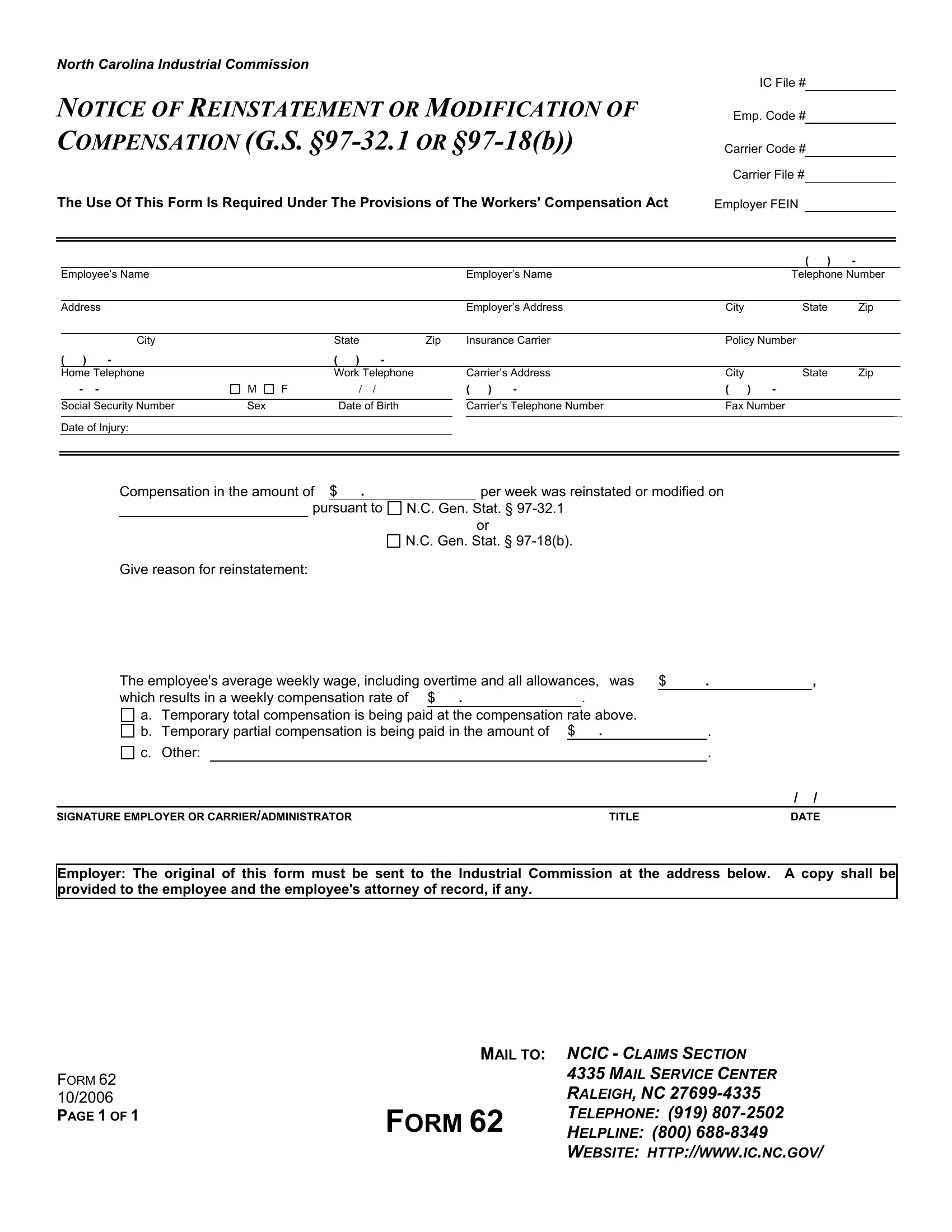
NORTH CAROLINA INDUSTRIAL COMMISSION
IC File #
NOTICE OF REINSTATEMENT OR MODIFICATION OF
COMPENSATION (G.S.
Emp. Code #
Carrier Code # Carrier File #
The Use Of This Form Is Required Under The Provisions of The Workers' Compensation Act |
Employer FEIN |
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
( ) |
- |
|
|
|
Employee’s Name |
|
|
|
|
|
|
Employer’s Name |
|
Telephone Number |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Address |
|
|
|
|
|
|
Employer’s Address |
City |
State |
Zip |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
City |
|
State |
|
Zip |
|
Insurance Carrier |
Policy Number |
|
|
|||
( ) |
- |
|
( |
) |
- |
|
|
|
|
|
|
|
|
|
|
Home Telephone |
|
Work Telephone |
|
|
Carrier’s Address |
City |
State |
Zip |
|
||||
- |
- |
M |
F |
/ |
/ |
|
( ) - |
( ) |
- |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
||||
|
Social Security Number |
Sex |
|
Date of Birth |
|
|
Carrier’s Telephone Number |
Fax Number |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of Injury:
Compensation in the amount of $ . |
|
per week was reinstated or modified on |
|
|
|
|
|
pursuant to |
N.C. Gen. Stat. § |
||
or
N.C. Gen. Stat. §
Give reason for reinstatement:
The employee's average weekly wage, including overtime and all allowances, was |
$ |
. |
, |
||||||
which results in a weekly compensation rate of $ |
. |
|
. |
|
|
|
|
||
|
|
|
|
|
|
|
|
||
a. Temporary total compensation is being paid at the compensation rate above. |
|
|
|
|
|||||
b. Temporary partial compensation is being paid in the amount of |
$ |
. |
|
|
. |
|
|||
c. Other: |
|
|
|
|
|
|
. |
|
|
|
|
|
|
|
|
|
/ |
/ |
|
SIGNATURE EMPLOYER OR CARRIER/ADMINISTRATOR |
|
|
TITLE |
|
|
DATE |
|||
Employer: The original of this form must be sent to the Industrial Commission at the address below. A copy shall be provided to the employee and the employee's attorney of record, if any.
|
MAIL TO: NCIC - CLAIMS SECTION |
|
FORM 62 |
|
4335 MAIL SERVICE CENTER |
|
RALEIGH, NC |
|
10/2006 |
|
|
PAGE 1 OF 1 |
FORM 62 |
TELEPHONE: (919) |
|
HELPLINE: (800) |
|
WEBSITE: HTTP://WWW.IC.NC.GOV/