
10-MSP can be completed online without difficulty. Simply make use of FormsPal PDF tool to complete the job in a timely fashion. In order to make our editor better and more convenient to work with, we constantly work on new features, taking into consideration feedback coming from our users. Should you be looking to get started, here is what it requires:
Step 1: First, access the editor by clicking the "Get Form Button" at the top of this site.
Step 2: With our advanced PDF editor, you are able to accomplish more than merely fill in blank form fields. Edit away and make your docs look perfect with customized text incorporated, or optimize the original input to excellence - all that accompanied by the capability to insert your personal images and sign the file off.
This document will need specific details to be filled out, so make sure you take some time to provide what's requested:
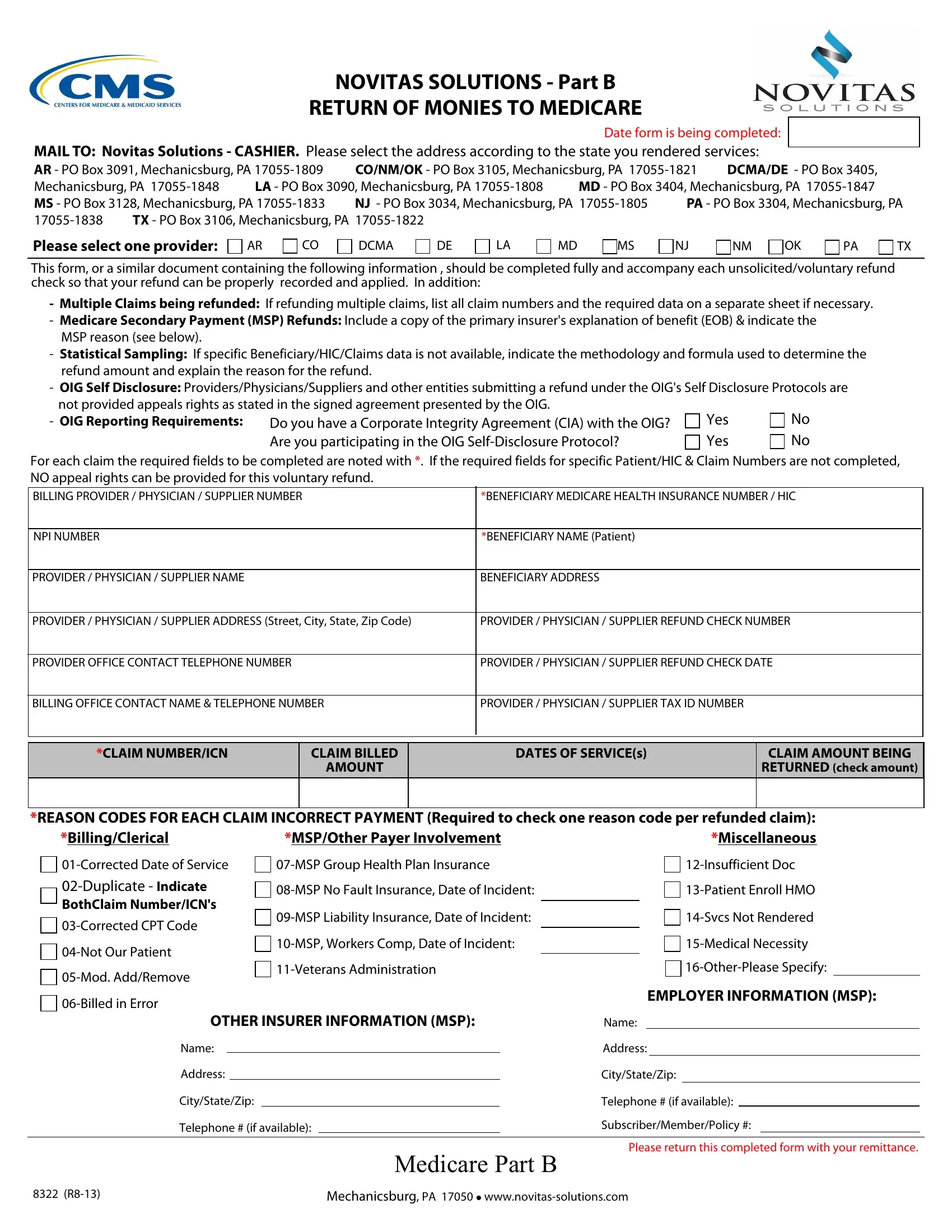
1. First of all, once completing the 10-MSP, begin with the area that features the next blank fields:
2. When this array of fields is finished, you should add the needed details in PROVIDER PHYSICIAN SUPPLIER NAME, BENEFICIARY ADDRESS, PROVIDER PHYSICIAN SUPPLIER, PROVIDER PHYSICIAN SUPPLIER, PROVIDER OFFICE CONTACT TELEPHONE, PROVIDER PHYSICIAN SUPPLIER, BILLING OFFICE CONTACT NAME, PROVIDER PHYSICIAN SUPPLIER TAX, CLAIM NUMBERICN, CLAIM BILLED, AMOUNT, DATES OF SERVICEs, CLAIM AMOUNT BEING RETURNED check, REASON CODES FOR EACH CLAIM, and MSPOther Payer Involvement in order to move forward further.
Always be very mindful when filling out MSPOther Payer Involvement and PROVIDER PHYSICIAN SUPPLIER, as this is the part where most people make errors.
3. The following part should also be rather simple, Address, CityStateZip, Telephone if available, CityStateZip, Telephone if available, SubscriberMemberPolicy, Mechanicsburg PA l, Medicare Part B, and Please return this completed form - these form fields will have to be filled out here.

Step 3: When you have looked again at the information in the file's blanks, just click "Done" to conclude your document generation. Find the 10-MSP the instant you register at FormsPal for a free trial. Conveniently gain access to the pdf file within your FormsPal account, along with any edits and changes being conveniently synced! At FormsPal.com, we strive to make sure that all your information is stored private.