Are you looking for a form to get started with Nucs 4556? It can be tricky navigating through all of the rules, regulations, and paperwork – especially if it's your first time doing so. But don't worry, we're here to help! Whether you're starting the registration process or just need some clarification on the forms and steps involved, this blog post will provide all of the detailed information you need about Nucs 4556. Read on to learn more about what it is, when to submit it, what documents are required - even how to find helpful resources along the way. Don't forget that having an understanding of these components upfront can make for a smoother experience in filling out and submitting your forms!
| Question | Answer |
|---|---|
| Form Name | Nucs 4556 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | nucs 4556, nevada detr employer power of attorney, where can i fax the nucs 4556 to, nevada form nucs 4556 |
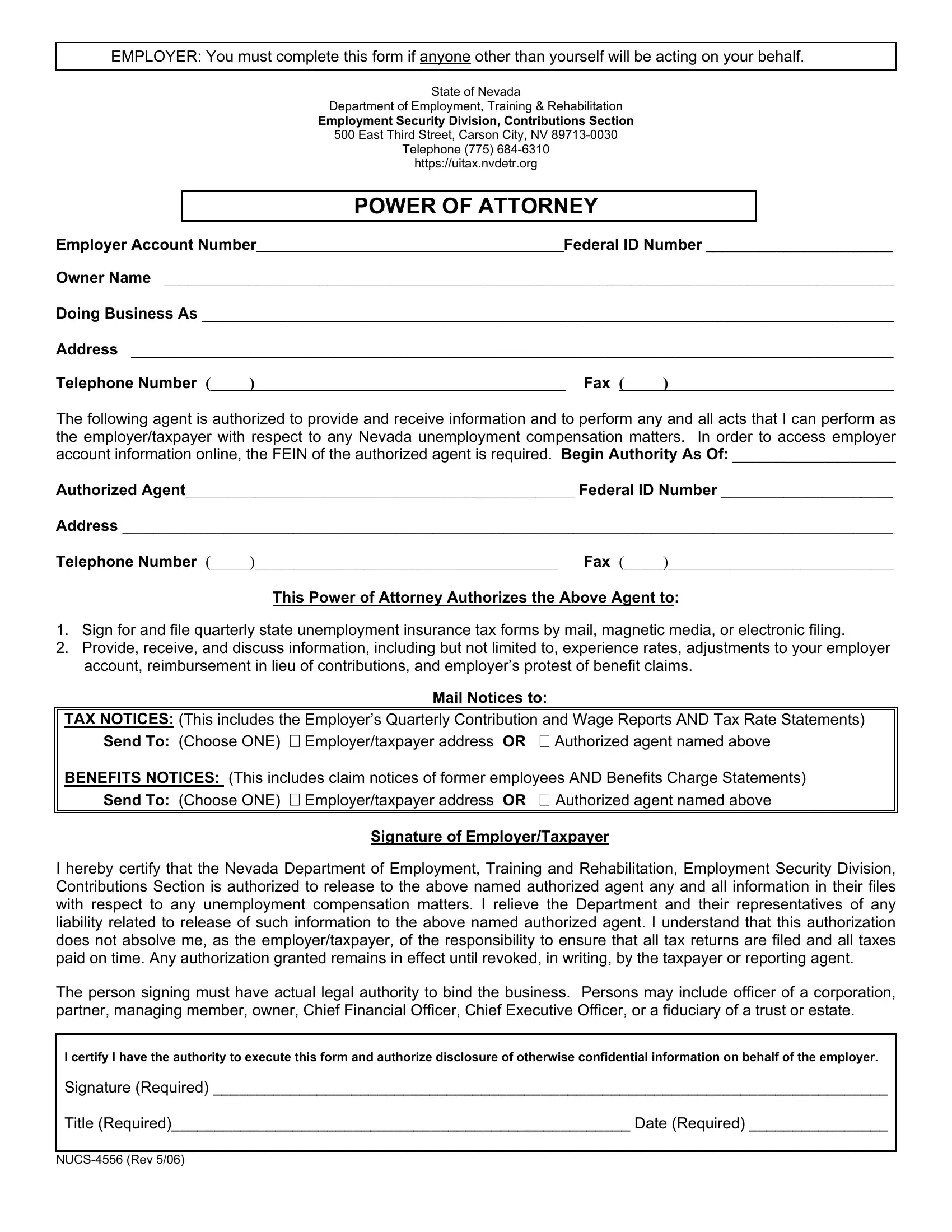
EMPLOYER: You must complete this form if anyone other than yourself will be acting on your behalf.
State of Nevada
Department of Employment, Training & Rehabilitation
Employment Security Division, Contributions Section
500 East Third Street, Carson City, NV
Telephone (775)
https://uitax.nvdetr.org
POWER OF ATTORNEY
Employer Account NumberFederal ID Number ________________________
Owner Name ______________________________________________________________________________________________
Doing Business As _________________________________________________________________________________________
Address __________________________________________________________________________________________________
Telephone Number (_____)_______________________________________ Fax (_____)_____________________________
The following agent is authorized to provide and receive information and to perform any and all acts that I can perform as the employer/taxpayer with respect to any Nevada unemployment compensation matters. In order to access employer account information online, the FEIN of the authorized agent is required. Begin Authority As Of: _____________________
Authorized Agent__________________________________________________ Federal ID Number ______________________
Address ___________________________________________________________________________________________________
Telephone Number (_____)_______________________________________ Fax (_____)_____________________________
This Power of Attorney Authorizes the Above Agent to:
1.Sign for and file quarterly state unemployment insurance tax forms by mail, magnetic media, or electronic filing.
2.Provide, receive, and discuss information, including but not limited to, experience rates, adjustments to your employer account, reimbursement in lieu of contributions, and employer’s protest of benefit claims.
Mail Notices to:
TAX NOTICES: (This includes the Employer’s Quarterly Contribution and Wage Reports AND Tax Rate Statements) Send To: (Choose ONE) Employer/taxpayer address OR
BENEFITS NOTICES: (This includes claim notices of former employees AND Benefits Charge Statements) Send To: (Choose ONE) Employer/taxpayer address OR Authorized agent named above
Signature of Employer/Taxpayer
I hereby certify that the Nevada Department of Employment, Training and Rehabilitation, Employment Security Division, Contributions Section is authorized to release to the above named authorized agent any and all information in their files with respect to any unemployment compensation matters. I relieve the Department and their representatives of any liability related to release of such information to the above named authorized agent. I understand that this authorization does not absolve me, as the employer/taxpayer, of the responsibility to ensure that all tax returns are filed and all taxes paid on time. Any authorization granted remains in effect until revoked, in writing, by the taxpayer or reporting agent.
The person signing must have actual legal authority to bind the business. Persons may include officer of a corporation, partner, managing member, owner, Chief Financial Officer, Chief Executive Officer, or a fiduciary of a trust or estate.
I certify I have the authority to execute this form and authorize disclosure of otherwise confidential information on behalf of the employer.
Signature (Required) ______________________________________________________________________________
Title (Required)_____________________________________________________ Date (Required) ________________