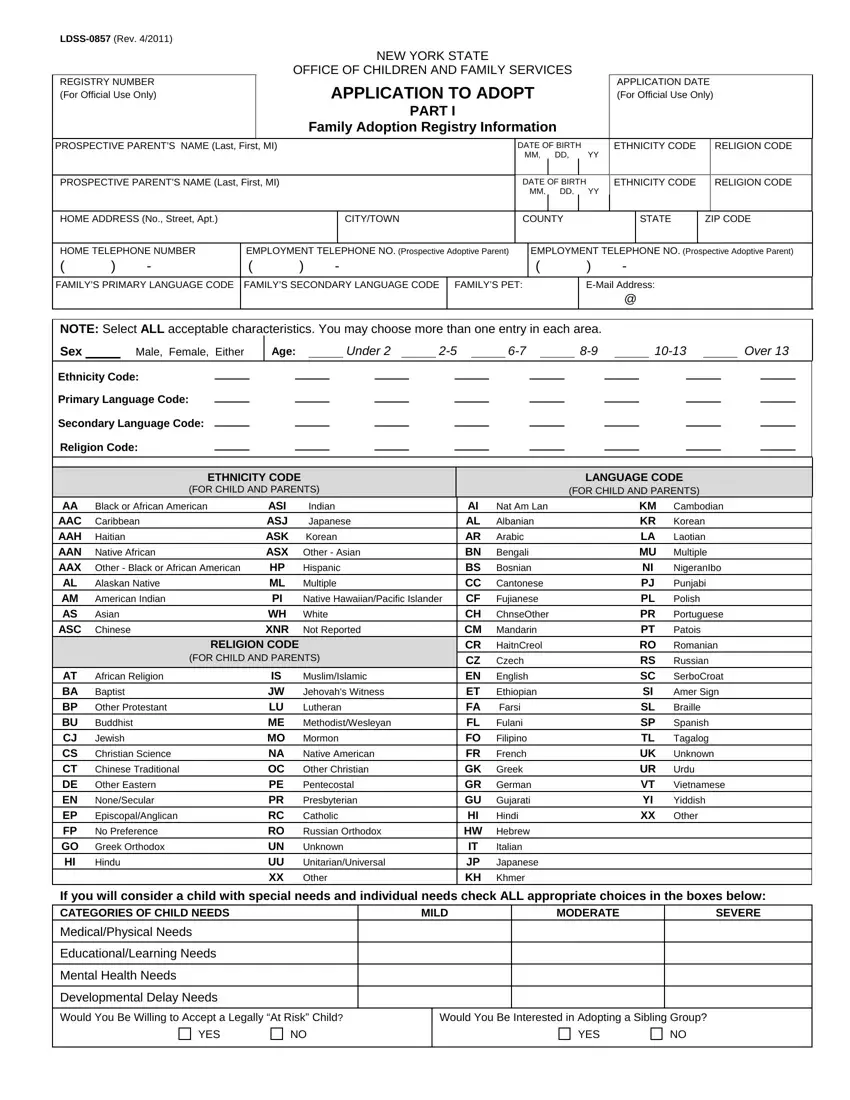
The New York State Adoption Form, officially known as LDSS-0857 (Rev. 4/2011), serves as an essential touchpoint for prospective adoptive parents navigating the adoption process. Crafted by the New York State Office of Children and Family Services, this comprehensive document embarks on gathering intricate details about prospective parents, aiming to facilitate a successful match between them and a child awaiting adoption. It categorizes essential personal information, including names, dates of birth, employment details, language preferences, and more, thus painting a detailed picture of the prospective adoptive family’s background. Additionally, the form thoughtfully inquires about the prospective parents' openness to embracing a child with specific characteristics such as age, gender, ethnicity, and special needs, indicating a commitment to accommodating the diverse needs and preferences of children in foster care. The adoption process’s complexity is further unpacked through sections that delve into the family’s home environment, their willingness to adopt siblings or children considered “at risk,” and the status of their homestudy process. Critical legal notes embedded within the form remind applicants of their rights and obligations, underline the importance of a thorough background check, and explain the procedure for seeking redress through a State administrative hearing should there be complications or concerns. This form not only serves as a gateway to the transformative journey of adoption but also underscores the state’s dedication to ensuring that the children’s best interests are at the forefront of all adoption proceedings.
| Question | Answer |
|---|---|
| Form Name | Ny Adoption Form |
| Form Length | 7 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 45 sec |
| Other names | ny 27 a form, 27a petition form, ny adoption form online, ny adoption a form |
