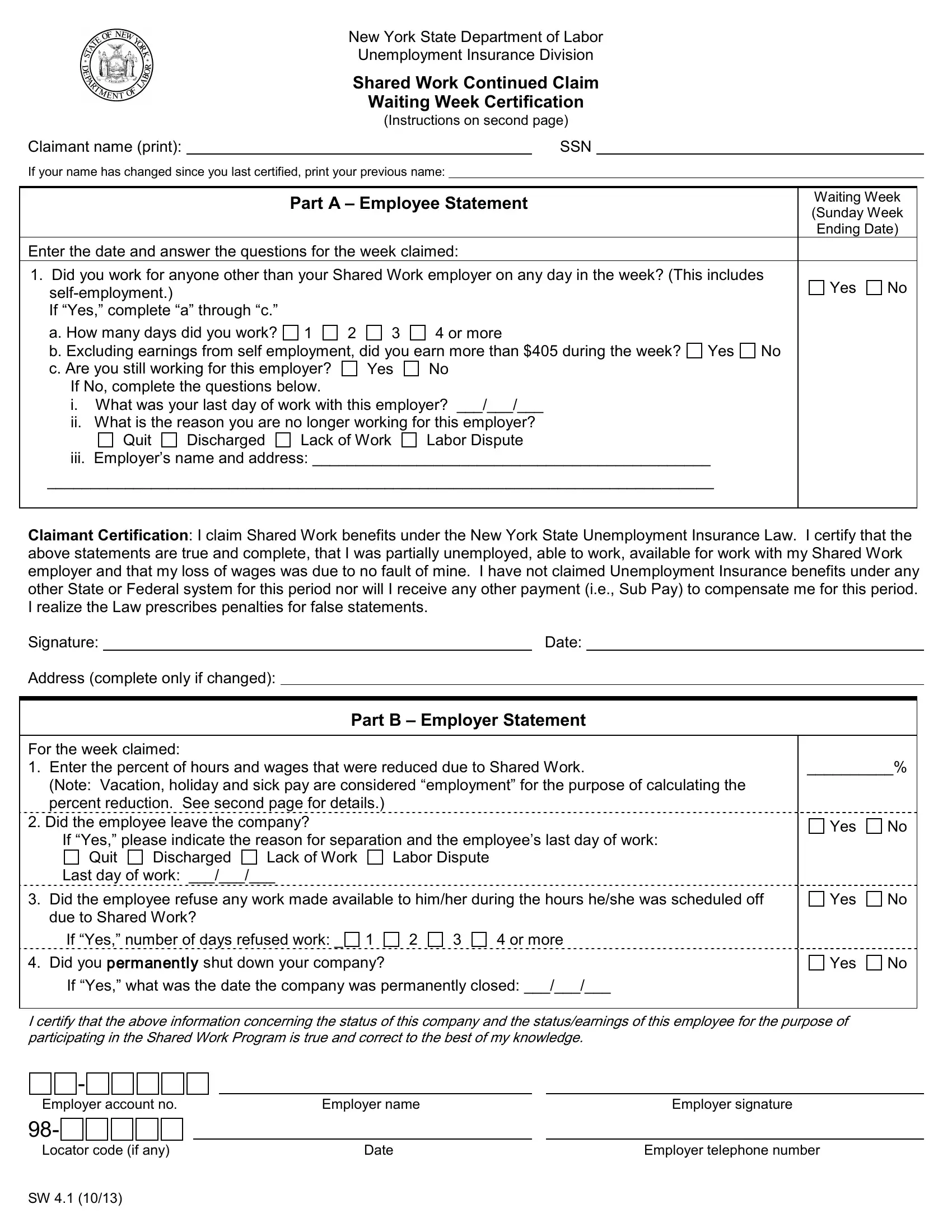
In the landscape of employment and labor laws, understanding the intricacies of unemployment insurance is crucial for both employers and employees navigating times of economic uncertainty. The New York State Department of Labor Unemployment Insurance Division's Shared Work Continued Claim form serves as a key document in this realm, facilitating a process by which employees can claim unemployment benefits during periods when their working hours are reduced under a shared work plan. This form is meticulously designed to capture essential information from the claimant, such as work history, earnings outside of shared work employment, and reasons for any reduction in hours or cessation of employment. Part A of the form requires detailed employee statements regarding their work status, any additional earnings, and personal attestations to their eligibility for shared work benefits. Conversely, Part B focuses on the employer’s perspective, demanding information on the reduction of hours and wages, work refusals, and the company's operational status. Coupled with instructions for both parties, the form’s structure aims to streamline the benefit claiming process, emphasizing accuracy, completeness, and timely submission to avoid delays in benefit dispensation. This straightforward yet comprehensive approach underscores the state’s commitment to supporting workers and employers alike in navigating shared work arrangements, thereby mitigating the financial impacts of reduced work schedules.
| Question | Answer |
|---|---|
| Form Name | Ny Labor Unemployment Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | SW4.1 unemployment labor form |
New York State Department of Labor
Unemployment Insurance Division
Shared Work Continued Claim
Waiting Week Certification
(Instructions on second page)
Claimant name (print): |
|
|
|
|
|
SSN |
|
|
|
|
If your name has changed since you last certified, print your previous name: |
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
Part A – Employee Statement |
Waiting Week |
||||||||
|
(Sunday Week |
|||||||||
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
Ending Date) |
||
Enter the date and answer the questions for the week claimed: |
|
|
|
|||||||
1. Did you work for anyone other than your Shared Work employer on any day in the week? (This includes |
Yes |
No |
||||||||
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
||
If “Yes,” complete “a” through “c.” |
|
|
|
|
|
|
|
|
|
|
a. How many days did you work? 1 |
2 |
3 |
4 or more |
|
|
|
||||
b. Excluding earnings from self employment, did you earn more than $405 during the week? Yes No |
|
|
|
|||||||
c. Are you still working for this employer? |
|
Yes |
No |
|
|
|
||||
If No, complete the questions below. |
|
|
|
|
|
|
|
|
|
|
i.What was your last day of work with this employer? ___/___/___
ii.What is the reason you are no longer working for this employer?
Quit |
Discharged |
Lack of Work |
Labor Dispute |
iii.Employer’s name and address: ______________________________________________
_____________________________________________________________________________
Claimant Certification: I claim Shared Work benefits under the New York State Unemployment Insurance Law. I certify that the above statements are true and complete, that I was partially unemployed, able to work, available for work with my Shared Work employer and that my loss of wages was due to no fault of mine. I have not claimed Unemployment Insurance benefits under any other State or Federal system for this period nor will I receive any other payment (i.e., Sub Pay) to compensate me for this period. I realize the Law prescribes penalties for false statements.
Signature: |
|
Date: |
|
|
Address (complete only if changed): |
|
|
|
|
Part B – Employer Statement
For the week claimed: |
|
|
|
|
|
|
||
1. |
Enter the percent of hours and wages that were reduced due to Shared Work. |
__________% |
||||||
|
(Note: Vacation, holiday and sick pay are considered “employment” for the purpose of calculating the |
|
|
|||||
|
percent reduction. See second page for details.) |
|
|
|
|
|
||
2. Did the employee leave the company? |
|
|
|
Yes |
No |
|||
|
If “Yes,” please indicate the reason for separation and the employee’s last day of work: |
|||||||
|
|
|
||||||
|
Quit |
Discharged |
Lack of Work |
Labor Dispute |
|
|
|
|
|
Last day of work: ___/___/___ |
|
|
|
|
|
||
3. |
Did the employee refuse any work made available to him/her during the hours he/she was scheduled off |
Yes |
No |
|||||
|
due to Shared Work? |
|
|
|
|
|
|
|
|
If “Yes,” number of days refused work: _ 1 |
2 |
3 |
4 or more |
|
|
||
4. |
Did you permanently shut down your company? |
|
|
|
Yes |
No |
||
|
If “Yes,” what was the date the company was permanently closed: ___/___/___ |
|
|
|||||
|
|
|
|
|
|
|
|
|
I certify that the above information concerning the status of this company and the status/earnings of this employee for the purpose of participating in the Shared Work Program is true and correct to the best of my knowledge.
-
Employer account no.Employer nameEmployer signature
98-
Locator code (if any) |
Date |
Employer telephone number |
SW 4.1 (10/13)
Shared Work Continued Claim
Part A - Instructions to Employee
This form is used to claim Shared Work benefits during a week(s) in which your normal hours of work were reduced according to a Shared Work Plan agreed to by your employer.
Complete Part A, “Employee Statement,” on the other side of this form. New York Unemployment Insurance benefit weeks run from Monday through Sunday. Be sure to show the Sunday week ending date(s) for the week(s) you wish to claim in the space provided at the top of the form.
If your name has changed, print your correct name and your previous name in the space provided at the top of the form.
If you have changed your address, print your new address in the space provided below your signature. Be sure to include your zip code.
Return this form to your employer, who will complete Part B and send it to the Department of Labor for processing.
Part B – Instructions to Employer
The purpose of this form is to confirm the status of employees you have listed in your Shared Work Plan.
The percent reduction is calculated by dividing the number of hours for which the employee was not paid due to work sharing by the number of hours normally worked in a week.
Shared Work benefits are not available for time that is paid for by the employer to the employee. That is, all time for which the employee receives compensation from the employer is considered “employment” for the purpose of calculating the percent reduction. This includes vacation, holiday and sick pay as well as payment for services performed.
Example: Employee’s normal schedule is 40 hours a week, 8 hours a day. Employer is shut down on Friday due to Shared Work.
a.Employee works Monday through Thursday: this is a 20% reduction.
b.Employee works Monday through Wednesday, gets paid sick leave for Thursday, is off Friday due to shutdown: this is a 20% reduction.
c.Employee works Monday through Thursday and gets holiday pay for Friday: this is a 0% reduction.
Give one form to each employee covered by your Shared Work Plan on the Monday following the latest Sunday week ending date on the reverse of the form, or as soon as possible thereafter if the employee is not working on Monday. This will be the second Monday after the date your Shared Work Plan becomes effective and every other Monday thereafter.
After the employee completes Part A and returns the form to you, complete Part B, “Employer Statement,” and send it to: NYS Department of Labor, Unemployment Insurance Division, Attention - Shared Work, PO Box 621, Albany, N.Y.
Mail the forms for all of the employees together in one envelope, if possible.
If you have a NY.GOV ID, you can send the forms by using the messaging feature after you log into your Unemployment Insurance Online Services account.
If the employee completed Part A and wishes to claim the week, submit the form for our review and determination even though you protest payment. Include a statement explaining why you protest the payment.
Review the completed form to be sure that it is correct.
Any errors or omissions will cause a delay in payment of benefits.
If you have questions, contact the Shared Work Unit at (518)