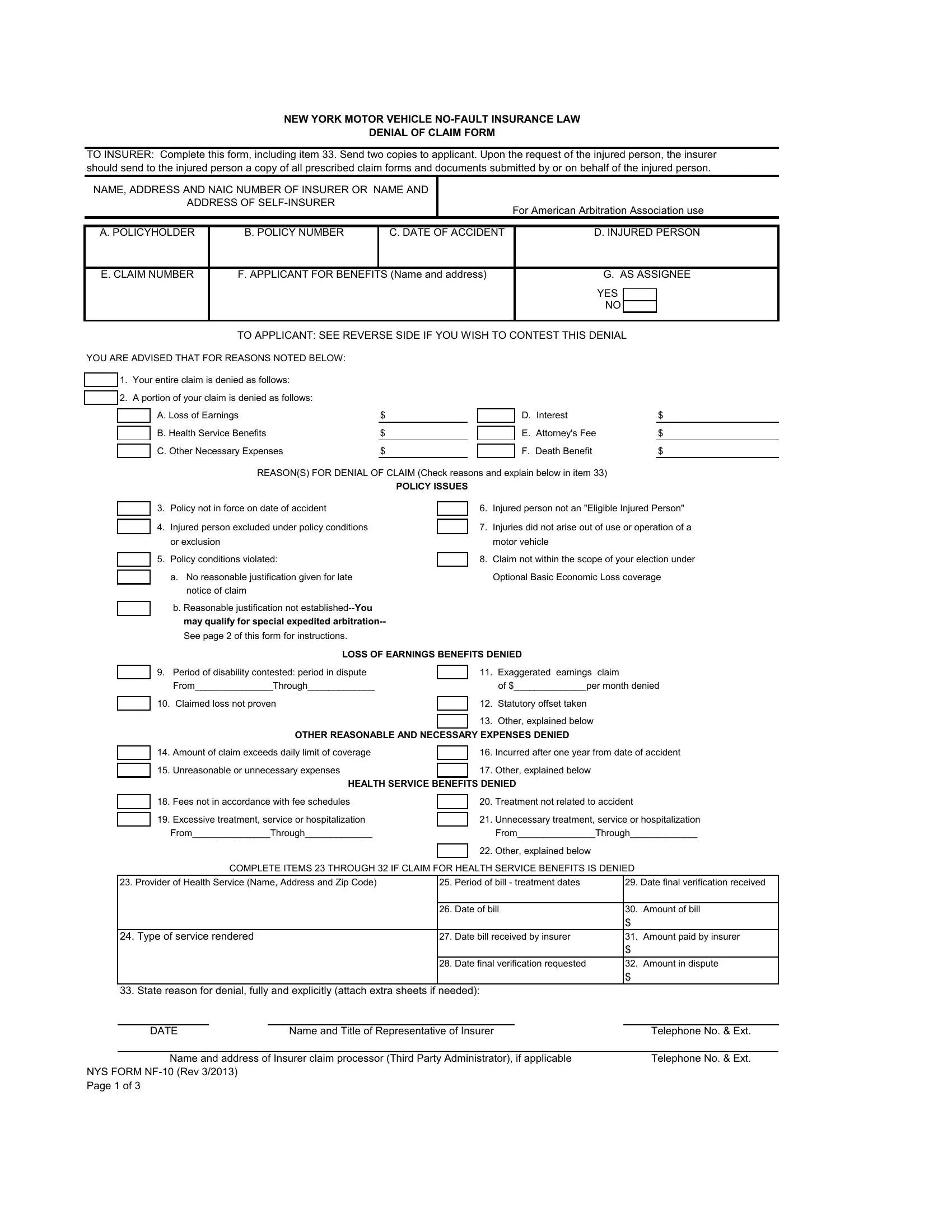
The New York State (NYS) NF-10 form plays a pivotal role in the realm of motor vehicle no-fault insurance, marking a critical juncture for policyholders and claimants navigating the complexities of claim denials. Designed to communicate an insurer's refusal to cover a claim under the New York Motor Vehicle No-Fault Insurance Law, this form ensures that clear, written notification is provided to the applicant or their assignee. It details the reasons for denial, whether it be for the entire claim or just a portion, specifying issues such as policy validity, policy exclusions, late notifications, and discrepancies in claimed losses, among others. The form not only outlines the grounds of the denial—ranging from loss of earnings and unreasonable medical expenses to disputes over the necessity and appropriateness of health services—but it also facilitates recourse for the aggrieved party. Through detailed instructions, it guides claimants on how to challenge the denial, whether by appealing to the New York State Department of Financial Services, engaging in arbitration with the American Arbitration Association, or pursuing legal action. In its essence, the NYS NF-10 form embodies the procedural fairness and transparency that underpin the adjudication of no-fault insurance claims, providing a structured pathway for both claim resolution and dispute escalation.
| Question | Answer |
|---|---|
| Form Name | Nys Form Nf 10 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | ny nf10, ny nf10 form, nf10, new york nf 10 form |