
With the online PDF tool by FormsPal, you can easily fill out or edit oaas pf 015 here and now. The editor is consistently upgraded by our team, getting new awesome functions and growing to be better. It merely requires a few simple steps:
Step 1: Access the form inside our editor by clicking on the "Get Form Button" above on this webpage.
Step 2: The editor enables you to work with your PDF form in a variety of ways. Enhance it by writing your own text, adjust original content, and place in a signature - all close at hand!
It will be an easy task to finish the form using out helpful tutorial! Here is what you have to do:
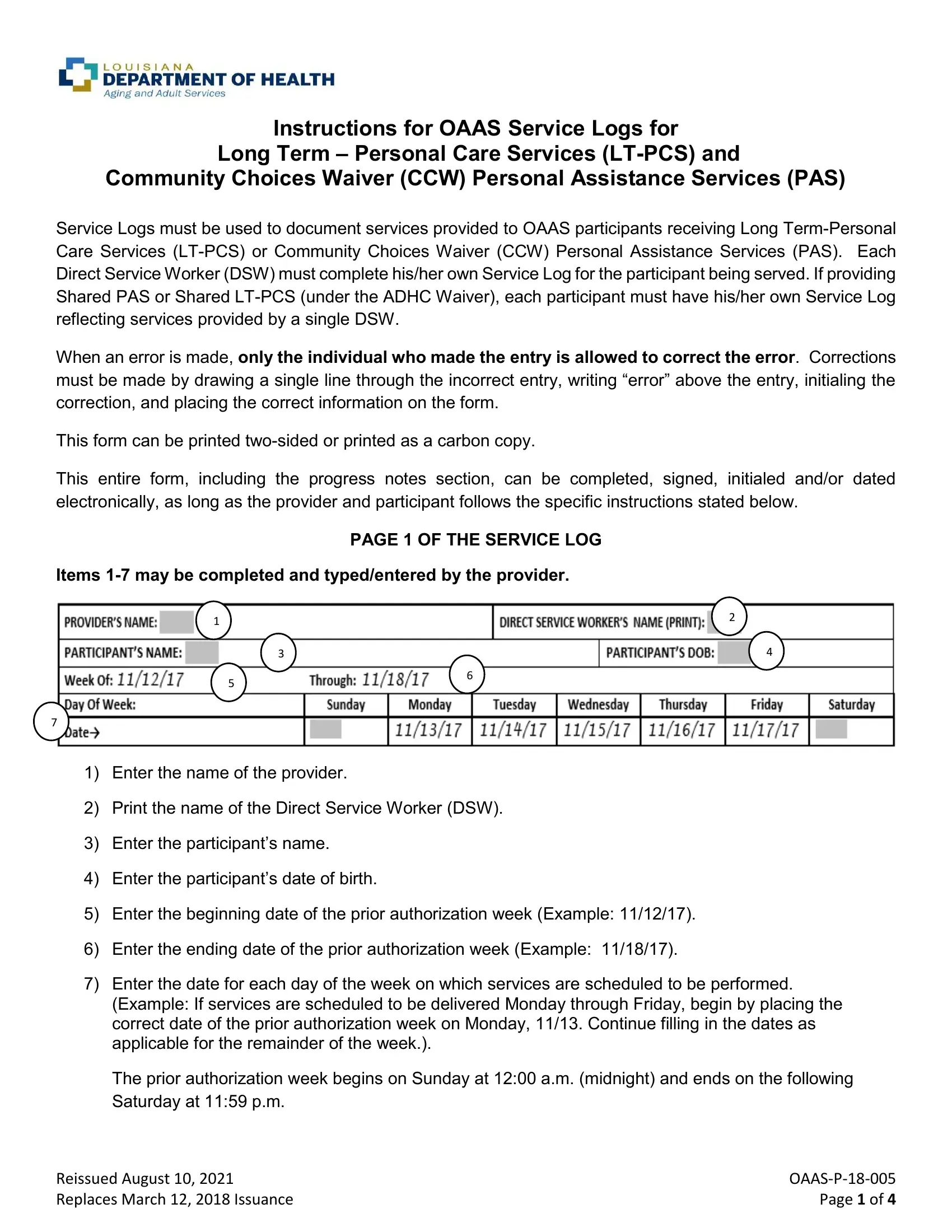
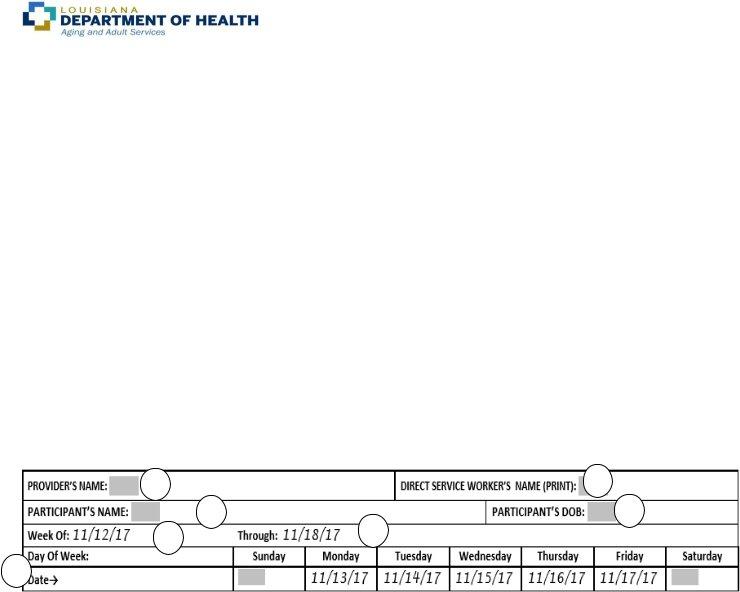
1. Start filling out your oaas pf 015 with a number of major blank fields. Collect all the necessary information and ensure nothing is omitted!
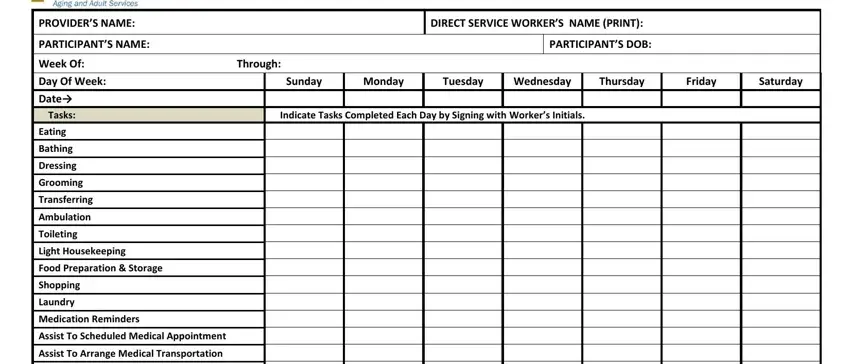
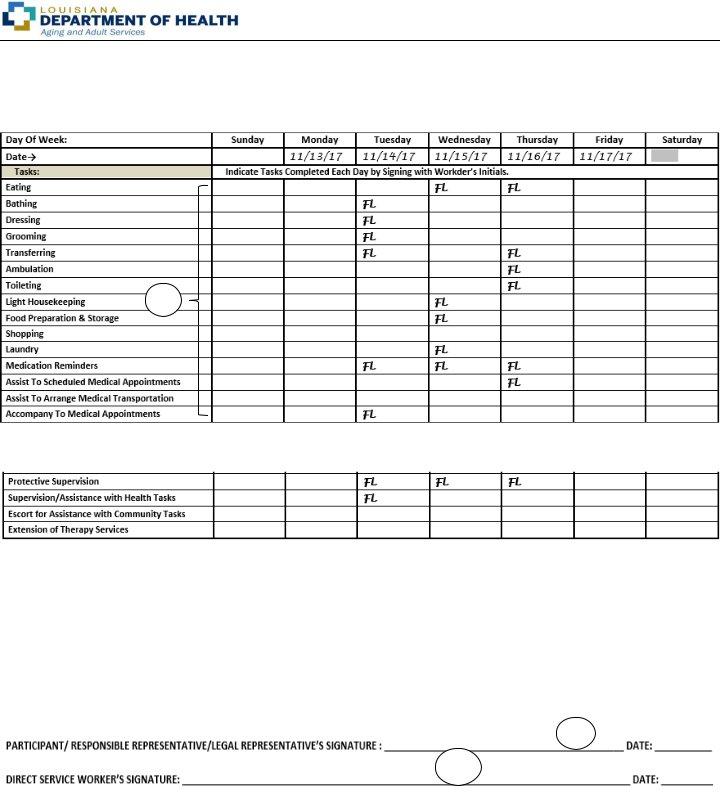
2. Just after performing the previous step, go on to the next stage and fill out the essential particulars in these blank fields - Accompany To Medical Appointments, Protective Supervision, SupervisionAssistance with Health, Escort for Assistance with, Extension of Therapy Services, PARTICIPANTRESPONSIBLE, NOTE TIMES OF SERVICE DELIVERY AS, DIRECT SERVICE WORKERS SIGNATURE, VERIFICATION EVV SYSTEM, Page of, Reissued August Replaces March, and OAASPF Page of.
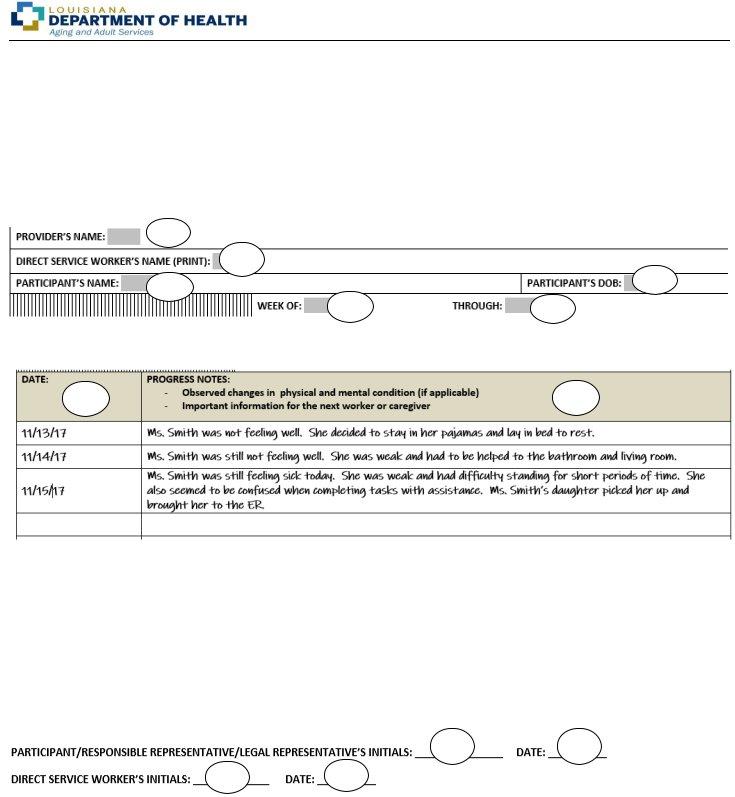
3. This third part should be fairly uncomplicated, NOTE THIS PAGE IS TO BE DUPLICATED, PROVIDERS NAME, DIRECT SERVICE WORKERS NAME PRINT, WEEK OF THROUGH, DATE, PROGRESS NOTES, Observed changes in physical and, and Important information for the next - these form fields will need to be completed here.
Be really mindful while completing WEEK OF THROUGH and Important information for the next, because this is the section where a lot of people make errors.
4. It's time to proceed to this fourth part! In this case you've got all these PARTICIPANTRESPONSIBLE, DIRECT SERVICE WORKERS INITIALS, Reissued August Replaces March, Page of, and OAASPF Page of fields to complete.
Step 3: Immediately after taking another look at your entries, hit "Done" and you're good to go! Acquire the oaas pf 015 after you subscribe to a 7-day free trial. Immediately view the pdf document in your FormsPal account page, along with any modifications and adjustments all synced! FormsPal is devoted to the personal privacy of all our users; we make certain that all information processed by our editor remains protected.