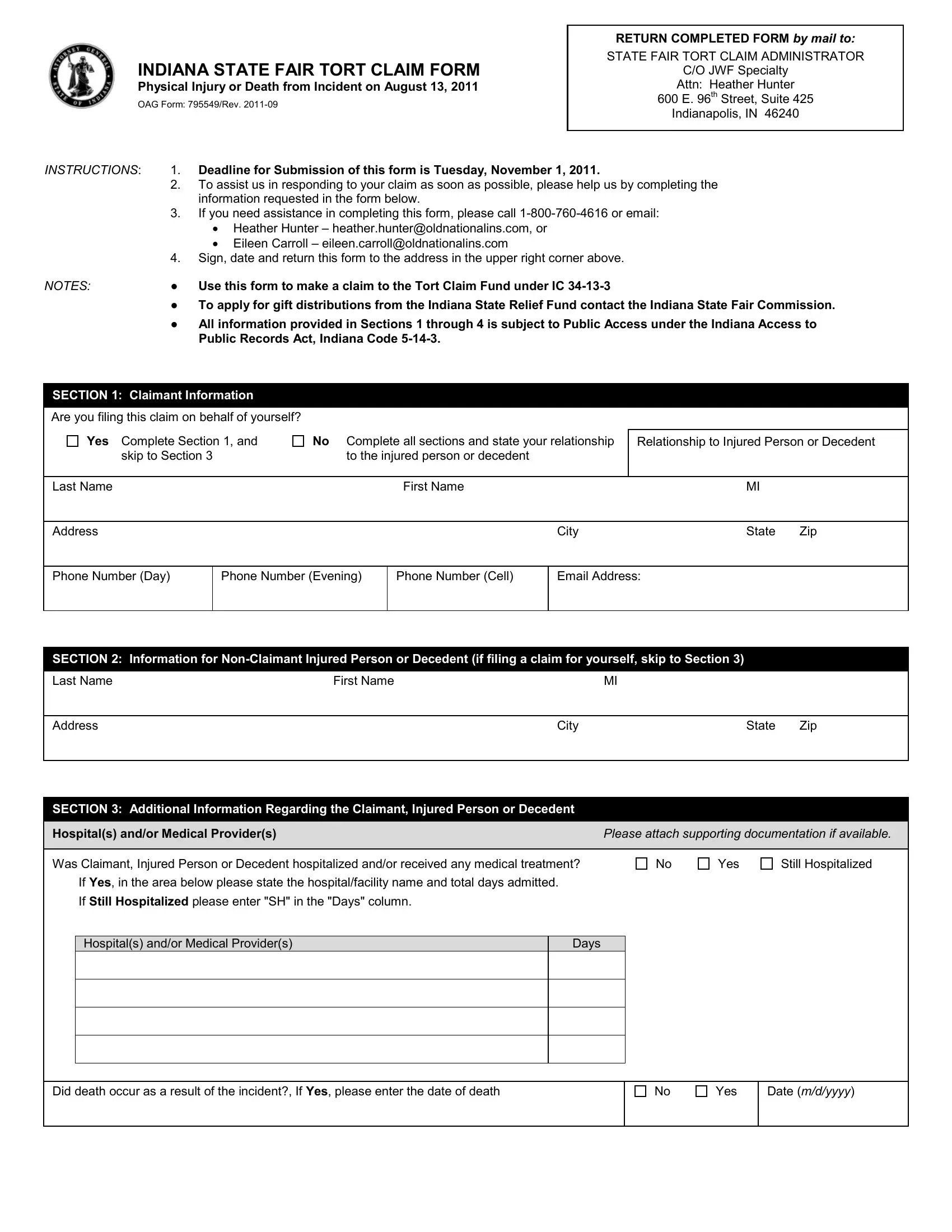
In the aftermath of the unfortunate incident on August 13, 2011, at the Indiana State Fair, the OAG 795549 form serves a crucial role in facilitating claims related to physical injuries or death. This detailed document, revised in September 2011, is a vital tool for individuals seeking to navigate the complexities of lodging a tort claim with the state. It outlines a clear process, starting from submission to the designated State Fair Tort Claim Administrator, housed at JWF Specialty under the attention of Heather Hunter in Indianapolis, Indiana. The form stipulates a submission deadline, underscoring the need for timely action. Moreover, it emphasizes the necessity of providing comprehensive information to assist in swift claim processing, offering guidance and support through contact information for assistance. As it navigates claimants through sections dedicated to personal information, details about the injured person or decedent, additional relevant information, and the method of payment, the form underscores the importance of transparency and accuracy. This is further highlighted by the requirement for claimants to certify the truthfulness and accuracy of the provided information, a step aimed at ensuring integrity in the claims process. Additionally, the form accommodates individuals' preferences for payment method, including an option for electronic fund transfer, demonstrating adaptability to modern needs while also providing an option to waive such requirements for those who prefer or require a traditional check payment. The OAG 795549 form ultimately represents a structured pathway for affected individuals to seek relief and compensation through the Indiana State Fair Tort Claim, reflecting the state's commitment to addressing the consequences of the tragic event.
| Question | Answer |
|---|---|
| Form Name | Oag Form 795549 |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | 96th, 2011, Eileen, tort claims examples |