When state and county agencies in Ohio require services from the Bureau of Motor Vehicles (BMV) and plan to pay through County Agency Voucher or Intra State Agency Voucher (ISTV), the Ohio BMV 0399 form emerges as a vital document. This form enables these agencies to formally request services while providing a structured way to include payment details. It's a concise process that mandates the inclusion of essential information such as the service requested, the date, detailed agency and customer/recipient information, the amount of the voucher/ISTV required, and any relevant BMV case numbers. The form further facilitates a smoother transition for revenue transfers by including a deadline—payments must be completed within 30 days post-service. Beyond this, it allows for attaching a voucher copy when applicable, and it underscores the importance of official authorization through a required agency authorized signature. Additionally, specific instructions for submitting the completed form are provided, ensuring that the process is navigated efficiently. By encompassing these features, the Ohio BMV 0399 form stands out as a key procedural element for facilitating necessary interactions between Ohio’s BMV and various state and county agencies.
| Question | Answer |
|---|---|
| Form Name | Ohio Form Bmv 0399 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | bmv0399 bmv 0399 form |
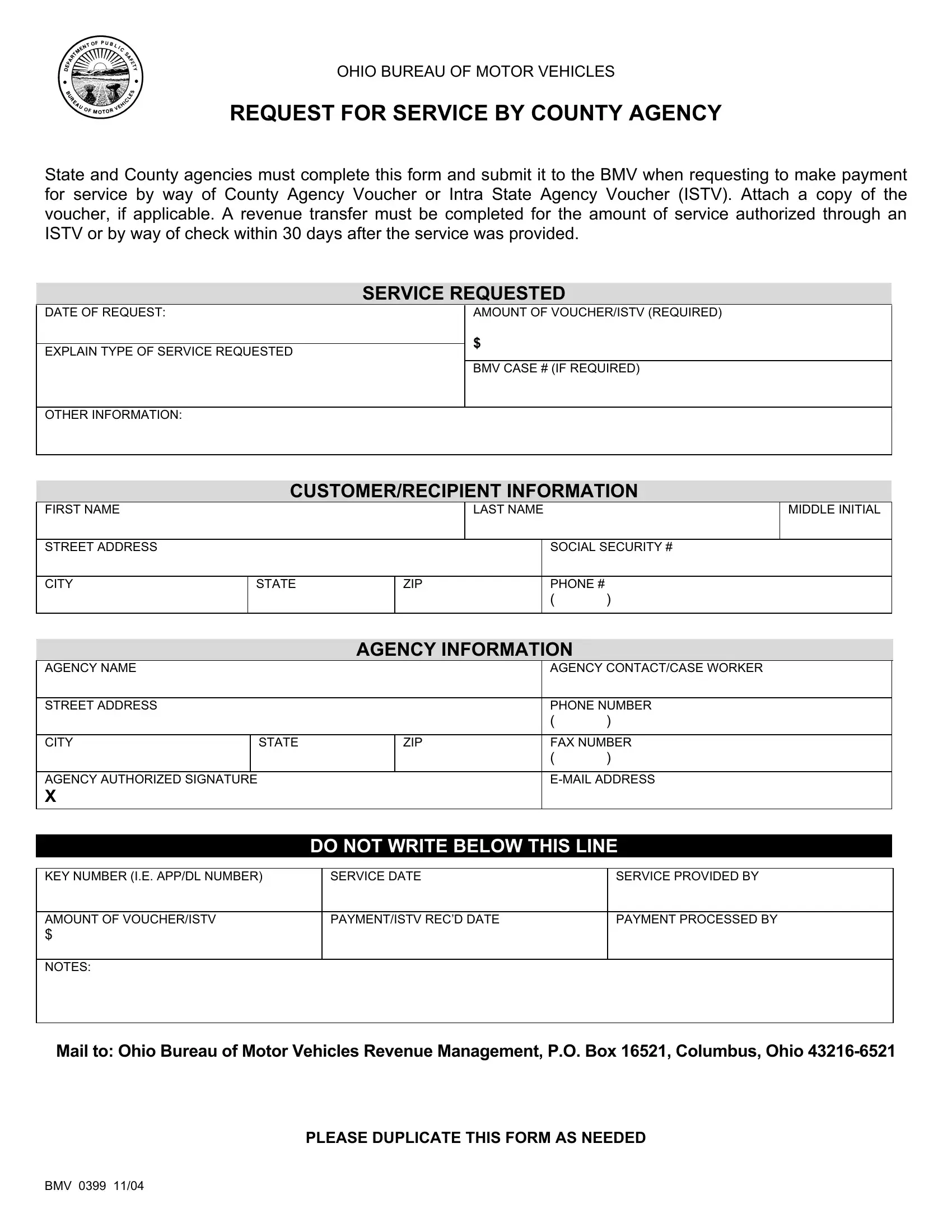
OHIO BUREAU OF MOTOR VEHICLES
REQUEST FOR SERVICE BY COUNTY AGENCY
State and County agencies must complete this form and submit it to the BMV when requesting to make payment for service by way of County Agency Voucher or Intra State Agency Voucher (ISTV). Attach a copy of the voucher, if applicable. A revenue transfer must be completed for the amount of service authorized through an ISTV or by way of check within 30 days after the service was provided.
SERVICE REQUESTED
DATE OF REQUEST:
EXPLAIN TYPE OF SERVICE REQUESTED
AMOUNT OF VOUCHER/ISTV (REQUIRED)
$
BMV CASE # (IF REQUIRED)
OTHER INFORMATION:
CUSTOMER/RECIPIENT INFORMATION
FIRST NAME |
|
|
LAST NAME |
|
|
MIDDLE INITIAL |
|
|
|
|
|
|
|
|
|
STREET ADDRESS |
|
|
|
|
SOCIAL SECURITY # |
||
|
|
|
|
|
|
|
|
CITY |
STATE |
ZIP |
|
PHONE # |
|
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
AGENCY INFORMATION
AGENCY NAME |
|
|
AGENCY CONTACT/CASE WORKER |
||
|
|
|
|
|
|
STREET ADDRESS |
|
|
PHONE NUMBER |
||
|
|
|
|
( |
) |
|
|
|
|
|
|
CITY |
|
STATE |
ZIP |
FAX NUMBER |
|
|
|
|
|
( |
) |
|
|
|
|
|
|
AGENCY AUTHORIZED SIGNATURE |
|
|
|||
X |
|
|
|
|
|
|
|
|
|
|
|
DO NOT WRITE BELOW THIS LINE
KEY NUMBER (I.E. APP/DL NUMBER) |
SERVICE DATE |
SERVICE PROVIDED BY |
|
|
|
AMOUNT OF VOUCHER/ISTV |
PAYMENT/ISTV REC’D DATE |
PAYMENT PROCESSED BY |
$ |
|
|
|
|
|
NOTES: |
|
|
|
|
|
Mail to: Ohio Bureau of Motor Vehicles Revenue Management, P.O. Box 16521, Columbus, Ohio
PLEASE DUPLICATE THIS FORM AS NEEDED
BMV 0399 11/04