
With the help of the online PDF editor by FormsPal, you can easily complete or edit Ohio Form Jfs 01296 right here. To make our editor better and less complicated to utilize, we constantly implement new features, with our users' feedback in mind. To get started on your journey, take these simple steps:
Step 1: Open the form inside our tool by clicking the "Get Form Button" above on this page.
Step 2: This editor gives you the capability to work with nearly all PDF documents in a variety of ways. Enhance it by writing personalized text, adjust existing content, and include a signature - all manageable in no time!
This PDF requires particular information to be typed in, thus make sure you take whatever time to enter exactly what is asked:
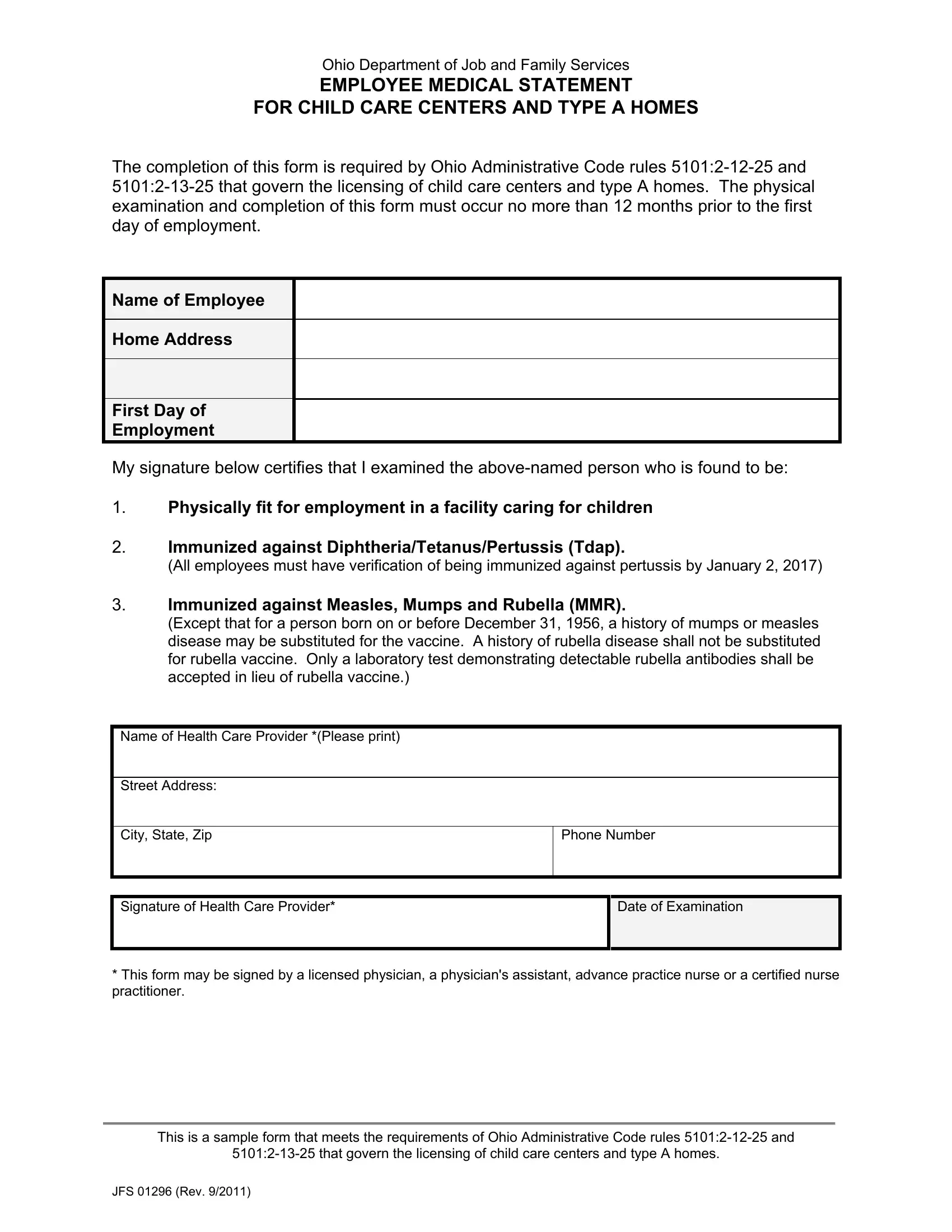
1. The Ohio Form Jfs 01296 will require specific information to be typed in. Ensure that the following blanks are complete:
2. Now that the previous section is done, you need to put in the necessary particulars in Name of Health Care Provider, Signature of Health Care Provider, Phone Number, Date of Examination, This form may be signed by a, and This is a sample form that meets so that you can progress further.
Those who use this form frequently get some points incorrect while filling in Name of Health Care Provider in this area. Remember to reread everything you type in here.
Step 3: Reread the information you've typed into the blank fields and click the "Done" button. Make a free trial plan at FormsPal and gain direct access to Ohio Form Jfs 01296 - download or modify from your FormsPal cabinet. We don't share the information you provide while working with documents at our site.