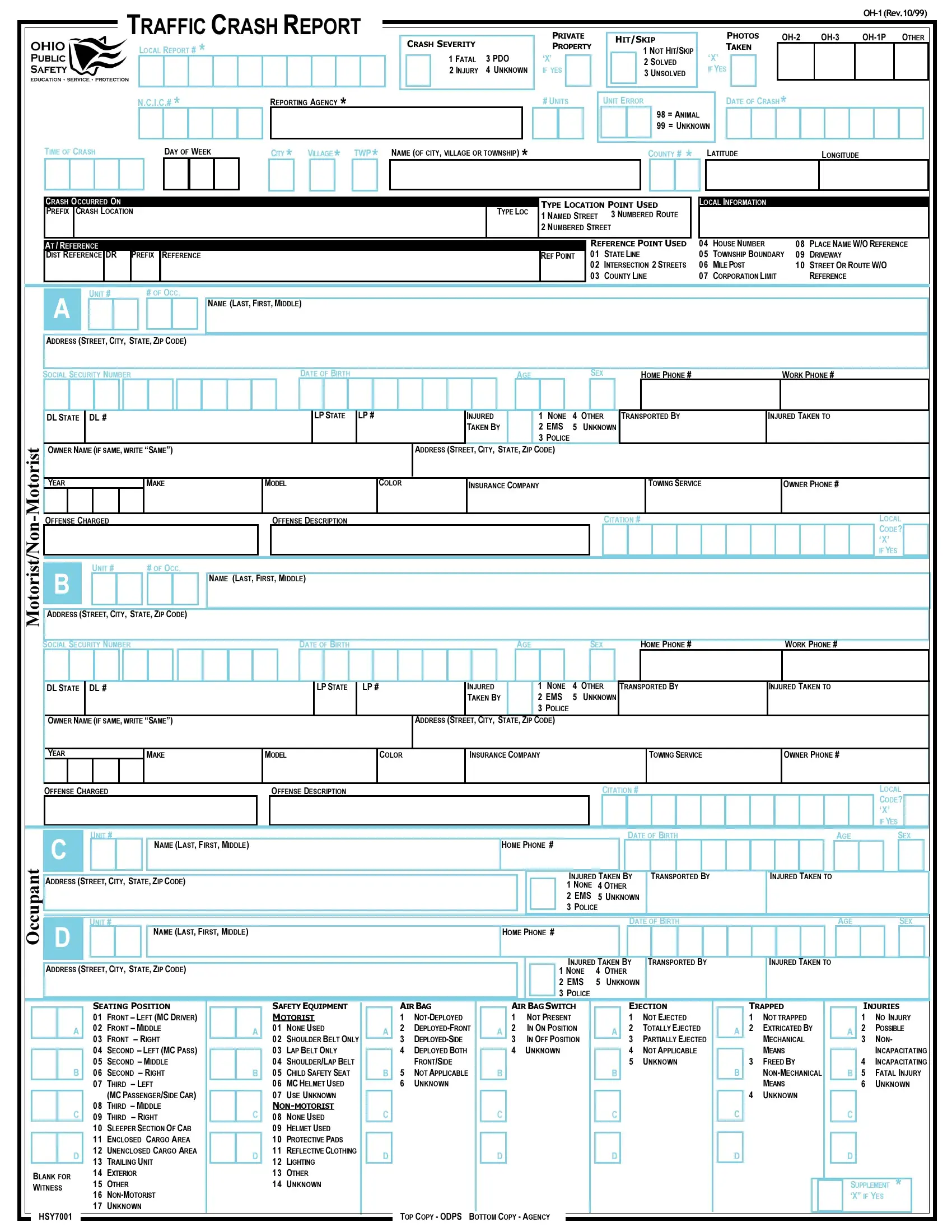

The Ohio Traffic Crash Report Form (OH-1) helps record specifics such as date, time, location, involved parties, and the sequence of events. It is important to follow the prescribed steps carefully to ensure the accuracy of this document.
1. Gather Required Information
Before starting the form, collect all necessary information. It includes driver details, vehicle information, insurance data, and specifics about the crash circumstances. Having all relevant documents and notes at hand will streamline the process.
2. Complete the Basic Information Section
Enter the date, time, and location of the crash. Make sure to provide accurate details as this sets the context for the report. Include street names, direction of travel, and any landmarks to identify the exact location of the accident.
3. Detail the Involved Parties
Fill out the sections related to drivers, passengers, pedestrians, or property owners involved in the crash. This part requires personal information, vehicle details, and insurance information for all parties involved.
4. Describe the Accident
Provide a detailed description of the accident. This covers the sequence of events leading up to the crash, the point of impact, and the aftermath. Use the diagram section to draw the positions of the vehicles before, during, and after the collision, if applicable.
5. Check Off Contributing Circumstances
Identify and mark any contributing factors to the accident. These can include weather conditions, road conditions, traffic signals, and driver behaviors such as speeding or failure to yield.
6. Add Witness Information
If there were any witnesses to the accident, include their statements and contact information. Witnesses can provide additional perspectives that might support the details of the crash report.
7. Review and Sign the Form
Once all sections are completed, review the information for accuracy and completeness. Any inaccuracies can affect legal proceedings and insurance claims. Sign the form to certify that the information provided is accurate.