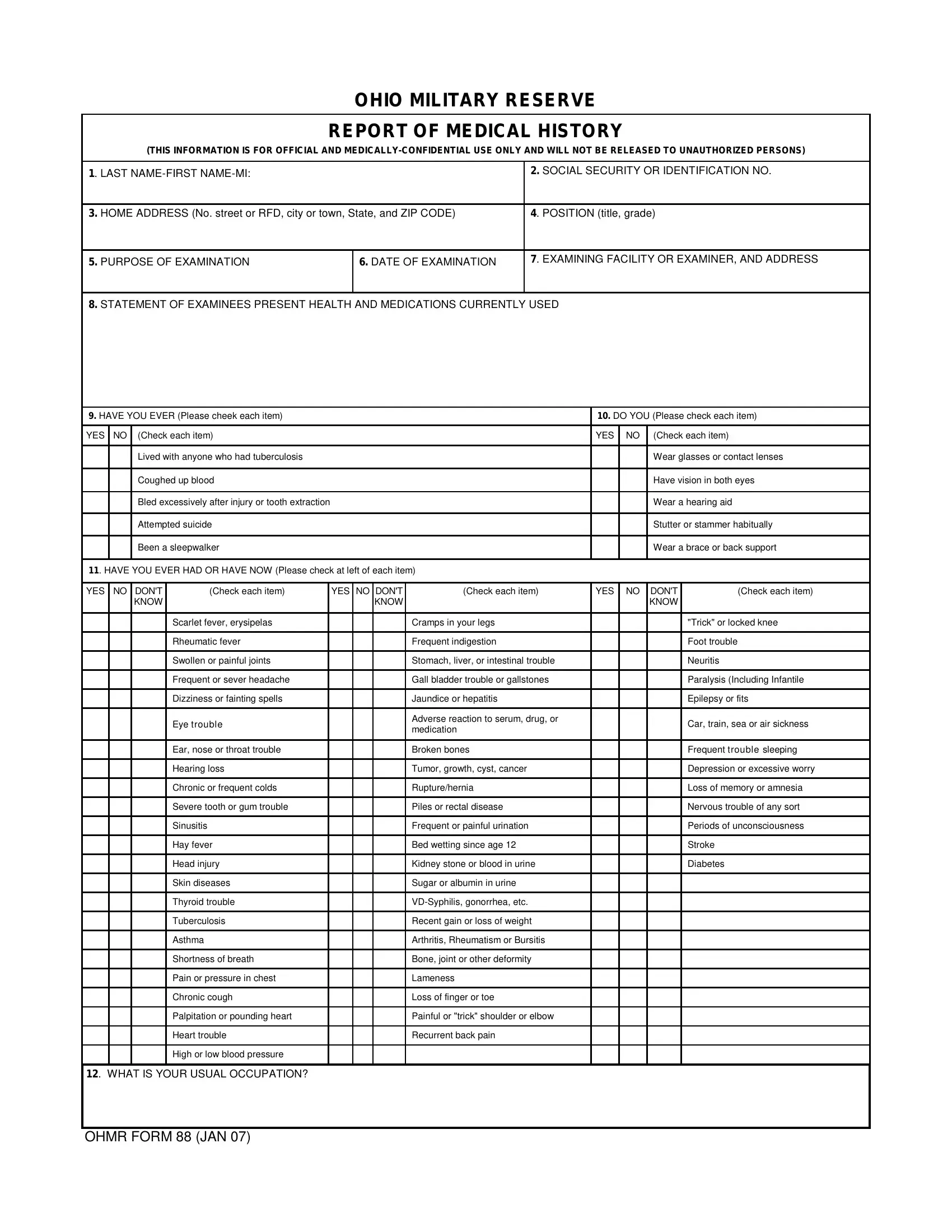
Understanding the OHMR 88 form, known officially as the Ohio Military Reserve Report of Medical History, is crucial for individuals seeking to serve in the Ohio Military Reserve. This document serves as a comprehensive health record, detailing an applicant's medical history, current health status, and any medical treatments or consultations received within the last five years. It is designed to glean a complete picture of the applicant's medical background, including any conditions that might affect their ability to serve. The form requires personal information, such as name, social security or identification number, home address, and the specific position the individual is applying for. Additionally, it covers a wide array of health-related queries, from past illnesses, surgeries, and hospital stays to questions about mental health, sensitivity to certain conditions, and even previous rejections from insurance or military service due to medical reasons. The OHMR 88 form is a critical document, ensuring that individuals are physically and mentally fit for service, while also safeguarding the health and safety of the service members. This confidential form also highlights the necessity for accuracy and truthfulness, with a declaration signed by the applicant affirming the veracity of the provided information, as well as consenting to the release of medical records for the application's assessment.
| Question | Answer |
|---|---|
| Form Name | Ohmr Form 88 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | ohmr88 ohmr form 88a |