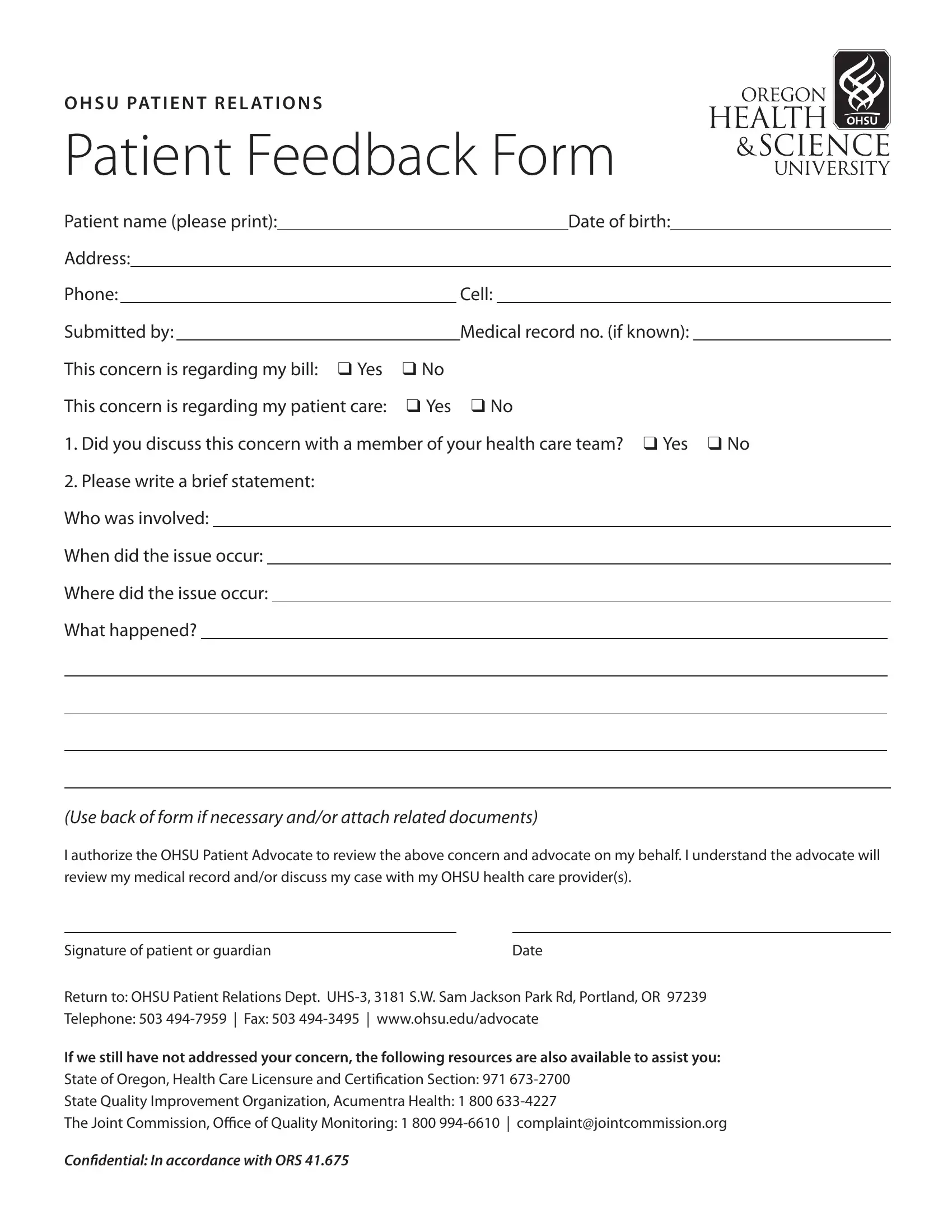
In the realm of healthcare, the voice of the patient is paramount, serving as a critical component for enhancing service quality and patient satisfaction. The Oregon Health & Science University (OHSU) understands this well, evidenced by the OHSU Patient Relations Patient Feedback Form. This document is a structured tool allowing patients to articulate their experiences, whether commendable or concerning, regarding their care or billing processes at OHSU. It requests essential information such as the patient's name, date of birth, address, contact numbers, and, if available, the medical record number. Notably, the form inquires if the issue is related to billing or patient care, encouraging patients to specify if they have previously attempted to resolve the matter with their healthcare team. Moreover, it prompts an explanation of the incident, including the who, when, and where, offering space for a detailed account and attachment of any pertinent documents. Significantly, the form includes an authorization for an OHSU Patient Advocate to intervene, emphasizing OHSU’s commitment to addressing patients' concerns. The document concludes by reminding patients of additional avenues for resolution, should their needs remain unmet, listing contact information for relevant state and national organizations. Through this comprehensive approach, OHSU not only facilitates a direct line of communication between patients and the institution but also underscores a broader commitment to accountability and continuous improvement in healthcare provision.
| Question | Answer |
|---|---|
| Form Name | Ohsu Patient Feedback Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | org, Oregon, patient feedback form pdf, patient feedback form |
OHSU PATIENT RELATIONS
PATIENT FEEDBACK FORM
Patient name (please print): |
|
|
|
|
|
Date of birth: |
|
||||
Address: |
|
|
|
|
|
|
|
||||
Phone: |
|
|
|
Cell: |
|
||||||
Submitted by: |
|
|
Medical record no. (if known): |
||||||||
|
|
|
|
|
|||||||
This concern is regarding my bill: ❑ Yes |
❑ No |
||||||||||
This concern is regarding my patient care: |
❑ Yes ❑ No |
||||||||||
1. Did you discuss this concern with a member of your health care team? ❑ Yes ❑ No
2.Please write a brief statement: Who was involved:
When did the issue occur: Where did the issue occur: What happened?
(Use back of form if necessary and/or attach related documents)
I authorize the OHSU Patient Advocate to review the above concern and advocate on my behalf. I understand the advocate will review my medical record and/or discuss my case with my OHSU health care provider(s).
Signature of patient or guardian |
Date |
Return to: OHSU Patient Relations Dept.
Telephone: 503
If we still have not addressed your concern, the following resources are also available to assist you:
State of Oregon, Health Care Licensure and Certiication Section: 971
State Quality Improvement Organization, Acumentra Health: 1 800
The Joint Commission, Oice of Quality Monitoring: 1 800
Conidential: In accordance with ORS 41.675