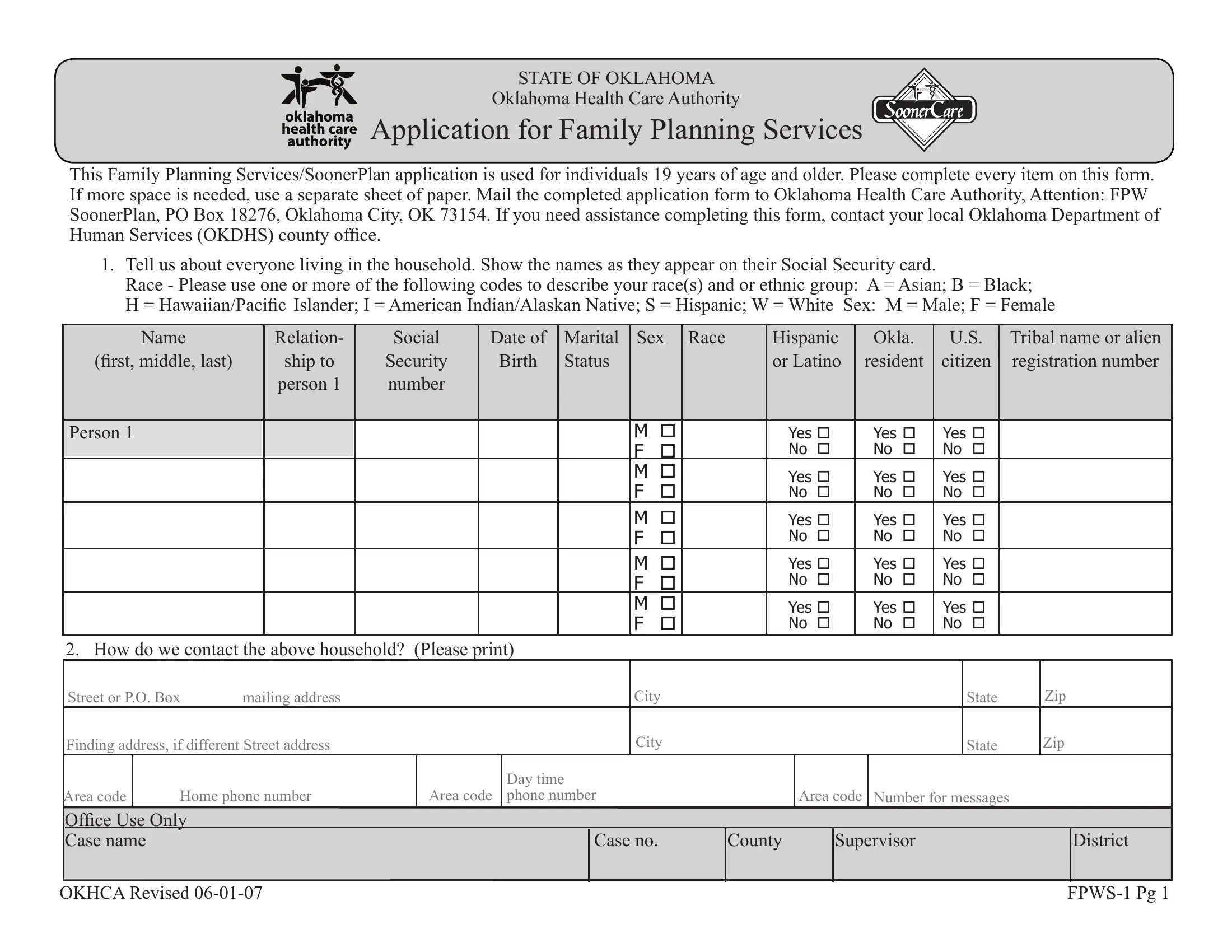
In today's healthcare landscape, the State of Oklahoma provides a crucial service through its Oklahoma Health Care Authority's Application for Family Planning Services, known colloquially as the FPWS 1 form. This form is designed for individuals aged 19 and older seeking access to family planning services under the SoonerPlan program. By requiring comprehensive input on household composition, contact information, verification of U.S. citizenship and identity, employment and income details, and insurance coverage, the application ensures that essential family planning resources are accessible to those in need. To streamline the process, applicants are guided to provide names as displayed on social security cards, diverse racial identifications, and detailed income sources, illustrating the state's dedication to accommodating a wide array of applicants. Additionally, the form underlines the importance of honesty and integrity, with specific sections dedicated to the rights and responsibilities of the applicant, including consent for the Oklahoma Health Care Authority to verify provided information and pursue necessary payments. This meticulous approach underscores Oklahoma's commitment to delivering equitable and comprehensive family planning services to its residents, emphasizing the necessity of accuracy and transparency in the application process.
| Question | Answer |
|---|---|
| Form Name | Oklahoma Form Fpws 1 |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | SoonerCare, OKDHS, soonerplan, FPWS-1 |