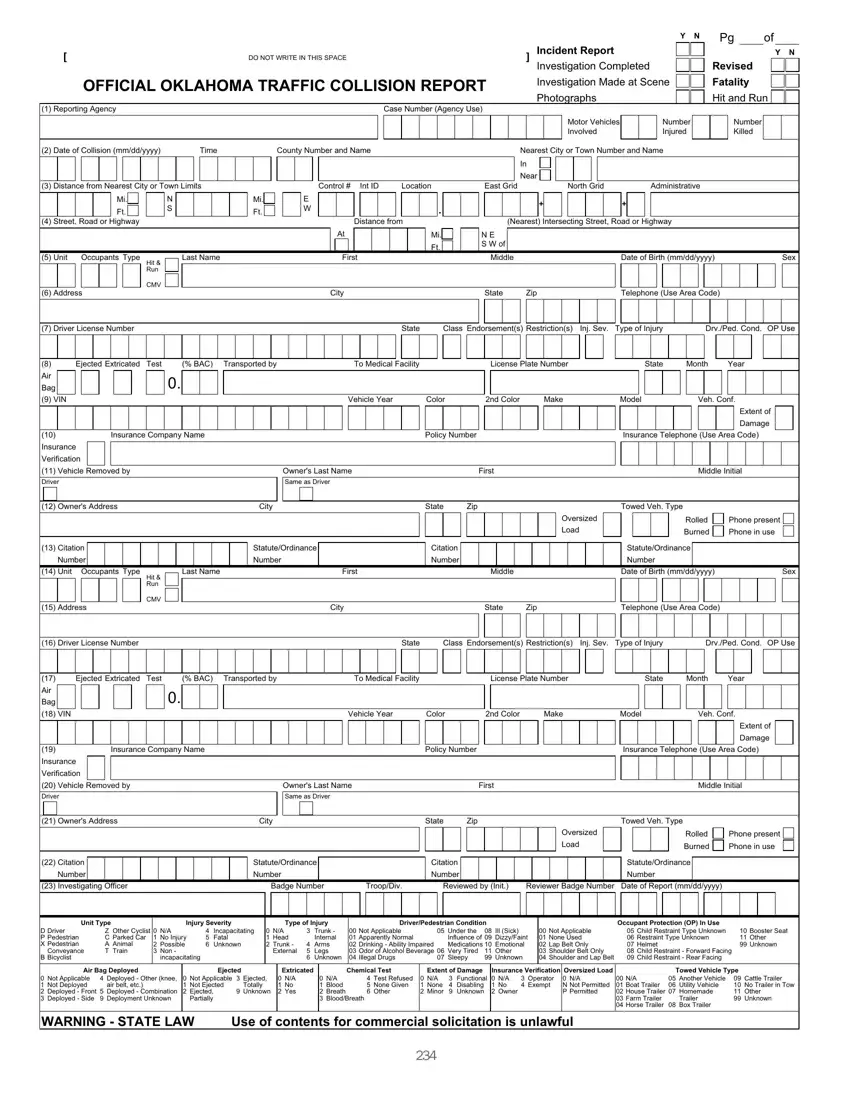
Completing this form accurately is crucial, as it is a legal document needed to document traffic incidents for investigations, insurance claims, and road safety data analysis.
1. Identify the Reporting Agency
Write the agency's name along with the investigating officer's badge number. If another officer reviews the form, their initials and badge number should also be included.
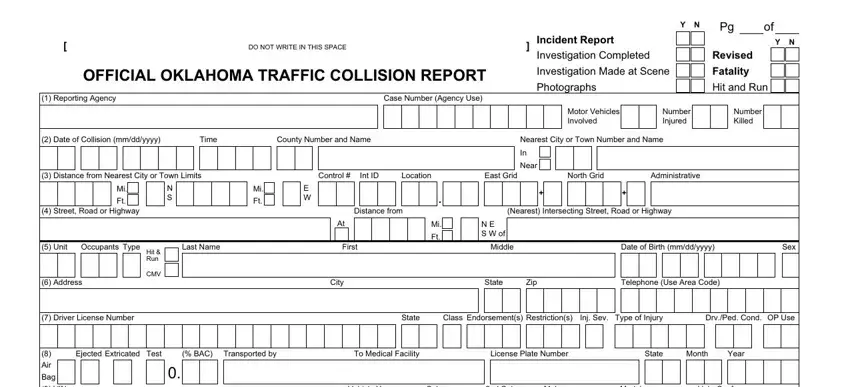
2. Document the Collision Details
Include the specific date and time of the collision. This is crucial for record-keeping and any potential legal proceedings. Also, you must specify the exact location, including the street or road, the distance from the nearest intersecting street, and the city or town nearest to the collision site.
3. Describe the Incident
In this section, detail the nature of the collision. Indicate whether it was a hit and run, involved property damage, or resulted in injuries or fatalities. If photographs were taken at the scene or an in-depth investigation was completed, note these details for a comprehensive event account.
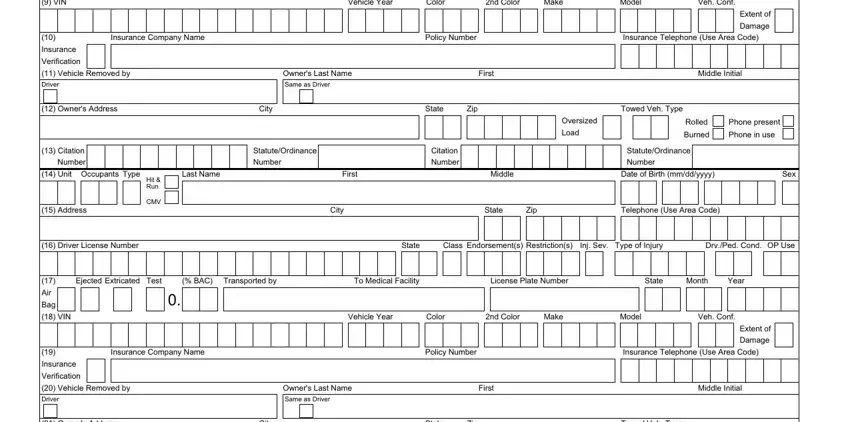
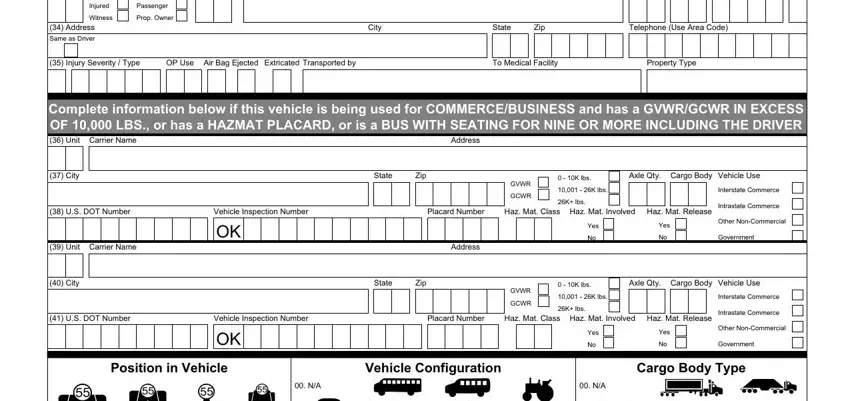
4. Vehicle and Driver Information
For each vehicle involved, provide a thorough description, including the make, model, color, year, and vehicle identification number (VIN). You must also document the driver’s information, such as name, address, date of birth, driver's license number, and any observable condition like impairment due to alcohol or drugs.
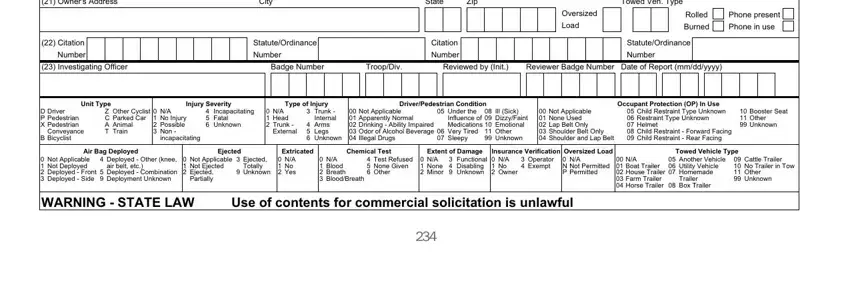
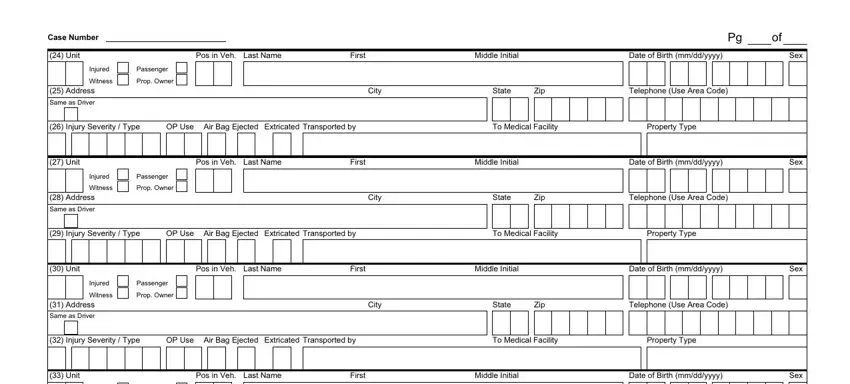
5. Record Occupant and Injury Information
Detail the number and type of occupants in each vehicle and describe the injuries sustained using the codes provided on the form. This information helps assess the collision's severity and impact (for emergency response and insurance claims).
6. Describe Weather and Road Conditions
The environmental and road conditions at the time of the accident can significantly influence the occurrence and outcome of traffic collisions. Record details like weather conditions, type of road surface, and any relevant traffic control devices that were in place or malfunctioned.
7. Official Use and Review
Ensure that all data entered is verified for accuracy and completeness. This section might require authorization or additional comments by the reviewing officer, especially if discrepancies or unusual circumstances surround the incident.
