
how to omh information can be filled out online without difficulty. Just try FormsPal PDF editing tool to accomplish the job without delay. The tool is consistently updated by our team, getting new functions and turning out to be better. If you're looking to start, here's what it takes:
Step 1: Click on the "Get Form" button in the top section of this page to access our PDF tool.
Step 2: With the help of this handy PDF tool, you may do more than merely fill in blanks. Try all the features and make your documents look great with custom textual content added, or fine-tune the original input to perfection - all that accompanied by the capability to add stunning pictures and sign the file off.
This form will need particular information to be entered, therefore ensure you take the time to fill in what's required:
1. Start filling out your how to omh information with a number of necessary blanks. Note all the important information and make certain there's nothing omitted!
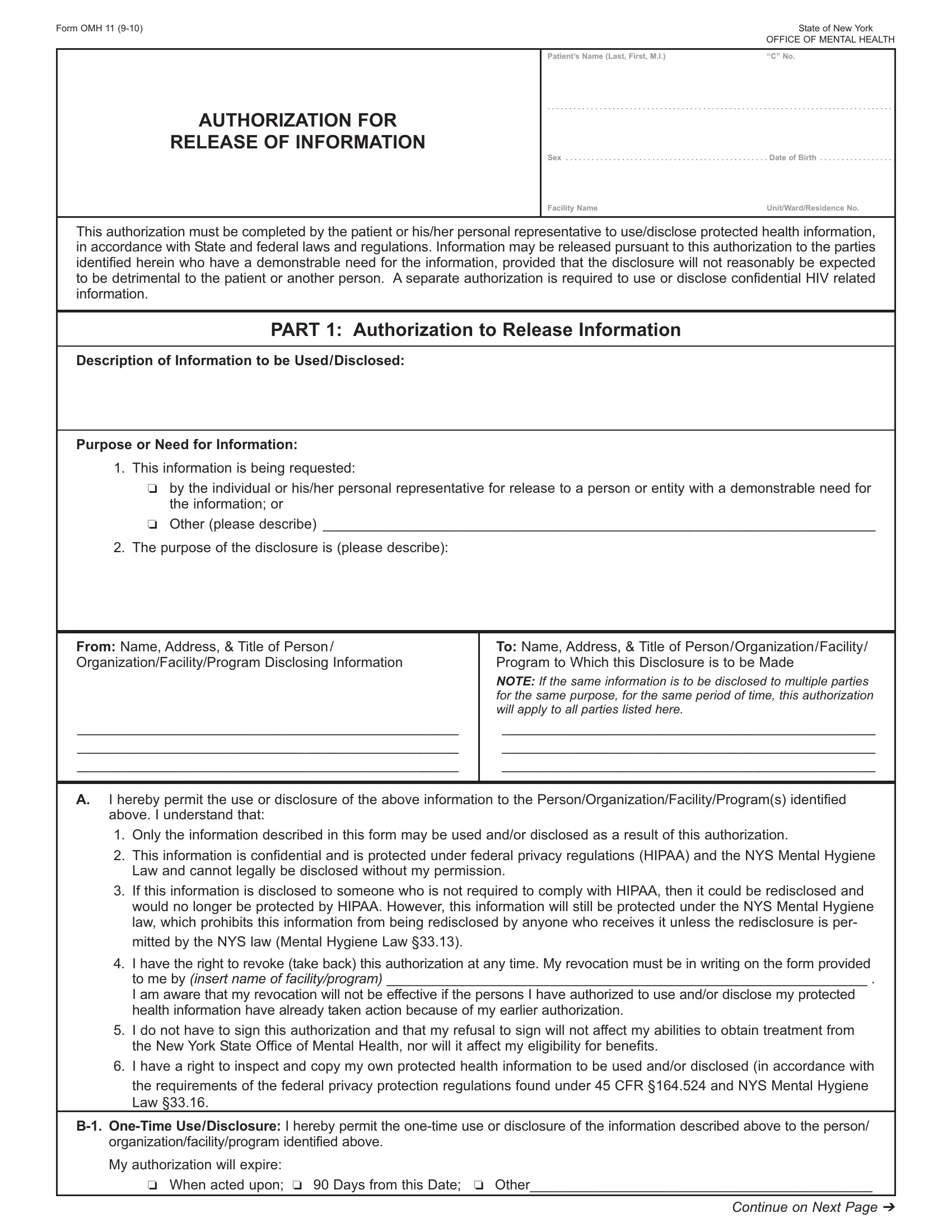
2. Soon after finishing the previous step, go on to the subsequent stage and enter the necessary particulars in all these blanks - Other please describe, The purpose of the disclosure is, From Name Address Title of Person, To Name Address Title of, NOTE If the same information is to, I hereby permit the use or, Only the information described in, This information is confidential, Law and cannot legally be, If this information is disclosed, would no longer be protected by, and I have the right to revoke take.
It's very easy to get it wrong while filling out the From Name Address Title of Person, and so be sure you reread it before you'll submit it.
3. This stage is usually straightforward - fill in every one of the blanks in I have the right to revoke take, I do not have to sign this, the New York State Office of, I have a right to inspect and, B OneTime UseDisclosure I hereby, organizationfacilityprogram, My authorization will expire, When acted upon Days from this, and Continue on Next Page to conclude this segment.
4. To go ahead, this fourth stage will require completing a handful of fields. These comprise of AUTHORIZATION FOR RELEASE OF, FacilityAgency Name, Patients Name Last First MI, OFFICE OF MENTAL HEALTH, CId No, B Periodic UseDisclosure I hereby, organizationfacilityprogram, My authorization will expire, When I am no longer receiving, One year from this date, Other, C Patient Signature I certify that, Signature of Patient or Personal, Date, and Patients Name Printed, which you'll find vital to carrying on with this document.
5. Because you near the completion of this document, there are actually several more requirements that should be met. Mainly, Date, To be Completed by Facility, Signature of Staff Person, Title, Date Released, PART Revocation of Authorization, I hereby revoke my authorization, and I hereby refuse to authorize the should be filled in.
Step 3: Right after you've looked once again at the information in the blanks, just click "Done" to finalize your form at FormsPal. Go for a 7-day free trial subscription with us and obtain direct access to how to omh information - downloadable, emailable, and editable from your personal cabinet. FormsPal offers risk-free form editor with no personal data record-keeping or distributing. Rest assured that your details are safe here!