
Using the online PDF editor by FormsPal, you can easily fill in or change how do you apply for handicap parking permit right here. In order to make our tool better and more convenient to utilize, we consistently come up with new features, with our users' suggestions in mind. With a few easy steps, you may begin your PDF editing:
Step 1: First of all, open the pdf editor by pressing the "Get Form Button" above on this site.
Step 2: Once you access the file editor, you will see the form all set to be filled in. Besides filling out different blanks, it's also possible to perform various other things with the PDF, namely adding your own textual content, editing the original text, inserting graphics, placing your signature to the PDF, and much more.
This document will require some specific details; in order to guarantee correctness, please make sure to adhere to the subsequent guidelines:
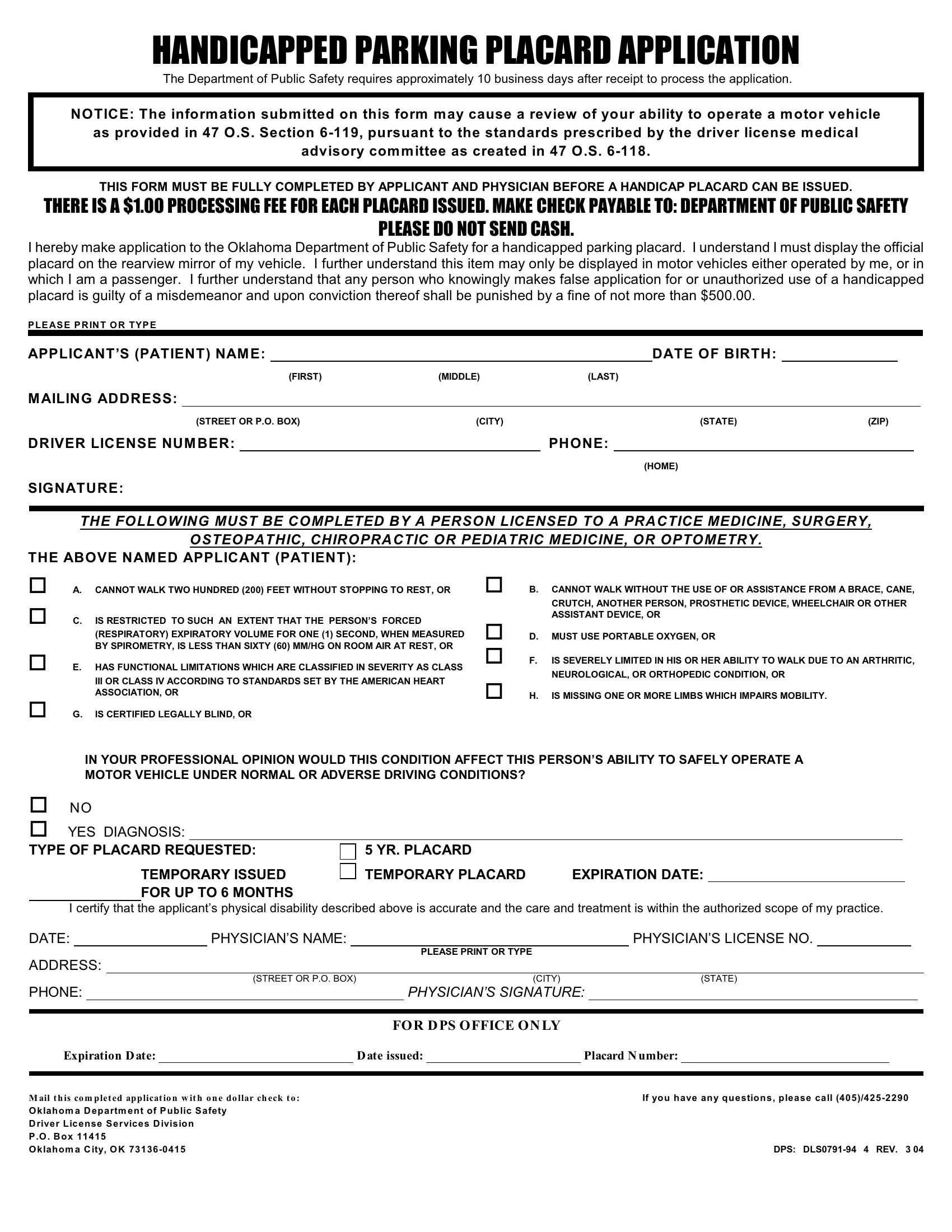
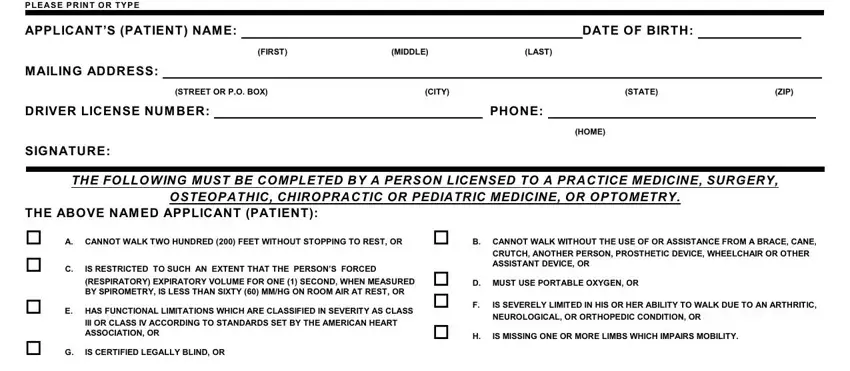
1. Firstly, when filling in the how do you apply for handicap parking permit, start in the section containing following blank fields:
2. After filling out this section, go on to the next stage and fill in the essential details in these fields - IN YOUR PROFESSIONAL OPINION WOULD, o NO o YES DIAGNOSIS TYPE OF, YR PLACARD TEMPORARY PLACARD, TEMPORARY ISSUED FOR UP TO MONTHS, I certify that the applicants, DATE PHYSICIANS NAME PHYSICIANS, ADDRESS, STREET OR PO BOX, CITY, STATE, PHONE PHYSICIANS SIGNATURE, PLEASE PRINT OR TYPE, Expiration D ate D ate issued, FOR D PS OFFICE ON LY, and M ail t h is co m plet ed applicat.
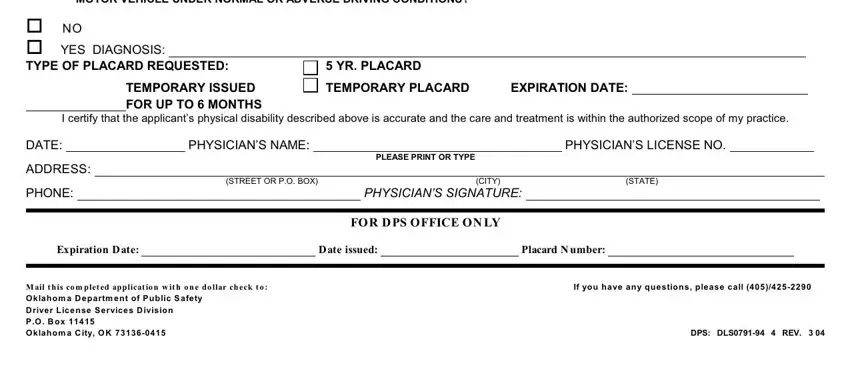
As for M ail t h is co m plet ed applicat and TEMPORARY ISSUED FOR UP TO MONTHS, be certain you do everything right in this section. These two could be the key fields in this PDF.
Step 3: After double-checking your fields, click "Done" and you are good to go! Right after getting a7-day free trial account here, it will be possible to download how do you apply for handicap parking permit or email it immediately. The file will also be at your disposal from your personal account page with all of your modifications. At FormsPal.com, we do our utmost to make certain that your information is stored private.