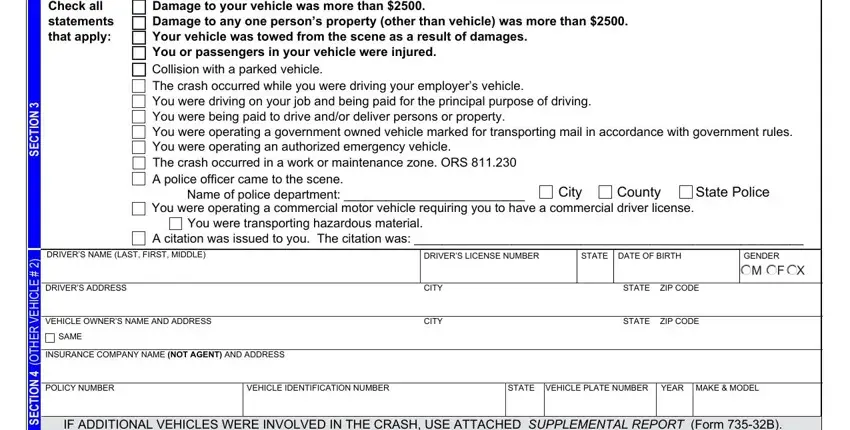
 Damage to your vehicle was more than $2500.
Damage to your vehicle was more than $2500. Damage to any one person’s property (other than vehicle) was more than $2500.
Damage to any one person’s property (other than vehicle) was more than $2500. Your vehicle was towed from the scene as a result of damages.
Your vehicle was towed from the scene as a result of damages.
 You or passengers in your vehicle were injured.
You or passengers in your vehicle were injured.
 Collision with a parked vehicle.
Collision with a parked vehicle.
 The crash occurred while you were driving your employer’s vehicle.
The crash occurred while you were driving your employer’s vehicle.
 You were driving on your job and being paid for the principal purpose of driving.
You were driving on your job and being paid for the principal purpose of driving.
 You were being paid to drive and/or deliver persons or property.
You were being paid to drive and/or deliver persons or property.
 You were operating a government owned vehicle marked for transporting mail in accordance with government rules.
You were operating a government owned vehicle marked for transporting mail in accordance with government rules. 
 You were operating an authorized emergency vehicle.
You were operating an authorized emergency vehicle.
 You were operating a commercial motor vehicle requiring you to have a commercial driver license.
You were operating a commercial motor vehicle requiring you to have a commercial driver license. 

 You were transporting hazardous material.
You were transporting hazardous material.
 A citation was issued to you. The citation was: ________________________________________________________
A citation was issued to you. The citation was: ________________________________________________________
 SAME
SAMEBy following these steps, you can successfully complete and submit the Oregon DMV Accident Report, ensuring compliance with state laws.
1. Verify the Requirement to File
Confirm that your accident meets the filing criteria, such as injury, death, significant property damage, or vehicle towing due to the crash. Understanding these requirements ensures compliance with Oregon law.
2. Gather Accident Information
Collect all necessary information about the accident, including date, time, location, vehicle details, driver details, and any witness information. This preparation streamlines the completion of the report.
3. Detail Accident Information
In the appropriate section, record the detailed specifics of the accident, including the exact date, time, and location. Accurate and precise details are essential for the DMV's records.
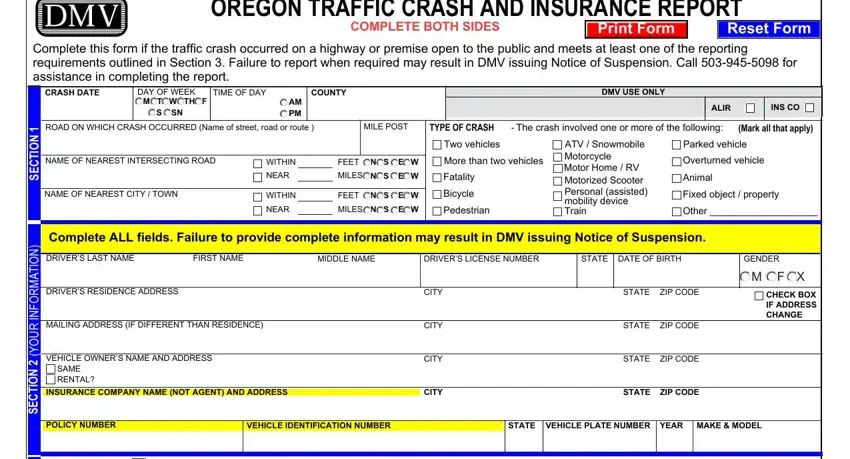
4. Describe Vehicles and Drivers Involved
For each vehicle involved, provide detailed descriptions, including make, model, year, VIN, and license plate number. Include comprehensive driver information such as name, address, and insurance details.
5. Document the Accident Scene
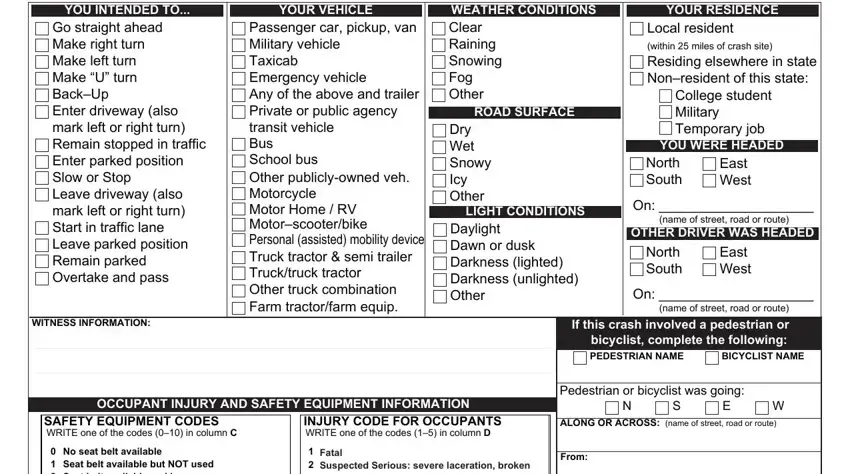
Fill in the section that requires information about the road conditions, weather, and lighting at the time of the accident. This data helps in analyzing the environmental factors influencing the accident.
6. Report Property Damage and Injuries
Document all damages to vehicles and other property, and list any injuries sustained by the involved parties. Precise documentation affects insurance claims and legal proceedings.
7. Complete Insurance Information
Enter insurance details for all parties involved in the accident. Incomplete or inaccurate insurance information can delay the report's processing and potential penalties.
8. Diagram the Accident
Draw a diagram on the provided space in the form, illustrating the positioning and movement of the vehicles at the time of the accident. This visual aid is crucial for understanding the dynamics of the crash.
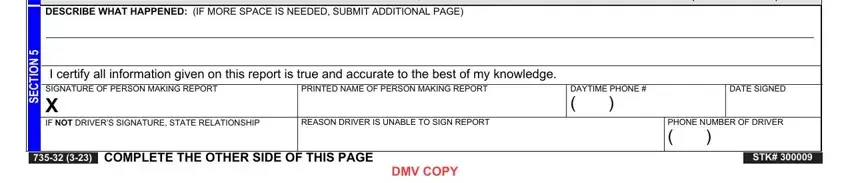
9. Review and Sign the Report
Review the entire form for accuracy and completeness. Sign the report to certify that all information provided is correct. This signature is a legal attestation to the truthfulness of the report.
10. Submit the Report
Decide on a method of submission — email, fax, mail, or delivery — and send the completed form to the DMV. Keep a copy of the submission confirmation as proof that you have met the legal requirements.
