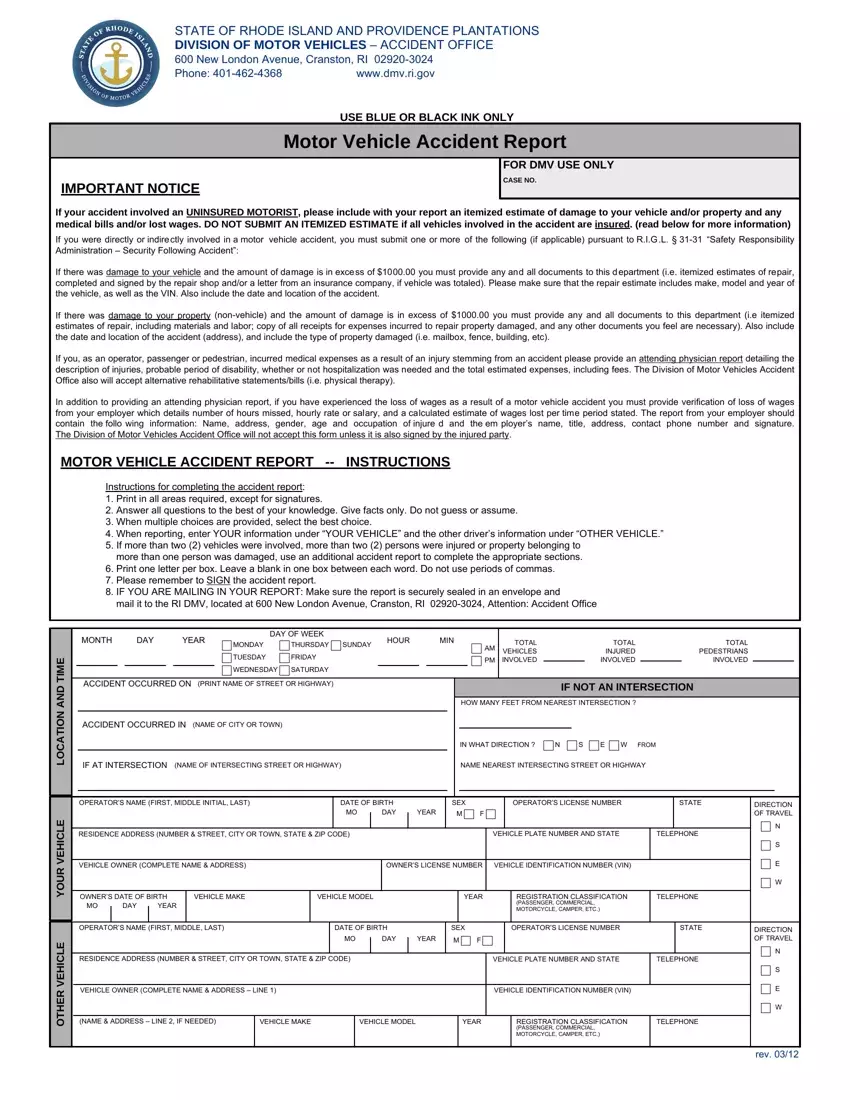
This guide assists persons involved in motor vehicle accidents in Rhode Island to complete the required Accident Report Form accurately.
1. Document Basic Information
Begin by entering the complete details of the accident location, including the name of the street or highway, the nearest intersecting street, and the city or town.
2. Fill in the Date and Time
Record the exact date and time of the accident. This information helps establish the sequence of events and is essential for insurance claims and legal documentation.
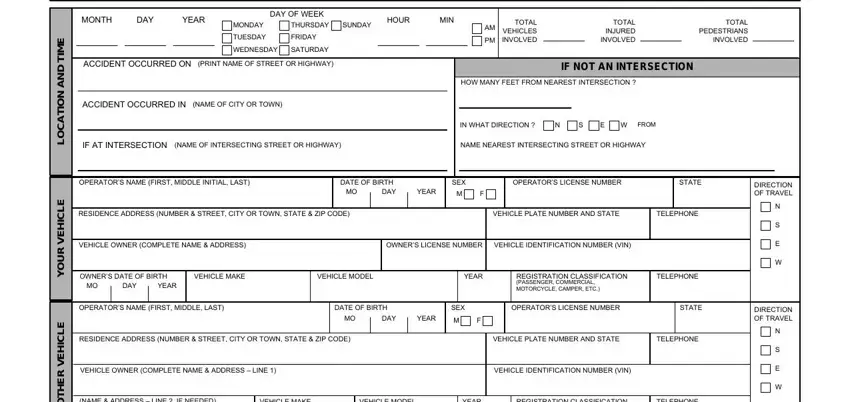
3. Vehicle and Driver Information
Detail the information regarding your vehicle under "YOUR VEHICLE" and the other vehicle under "OTHER VEHICLE." Include each vehicle's make, model, year, vehicle identification number (VIN), and license plate number. Also, provide the full name, date of birth, and driver’s license number for each driver involved.

4. Describe the Accident
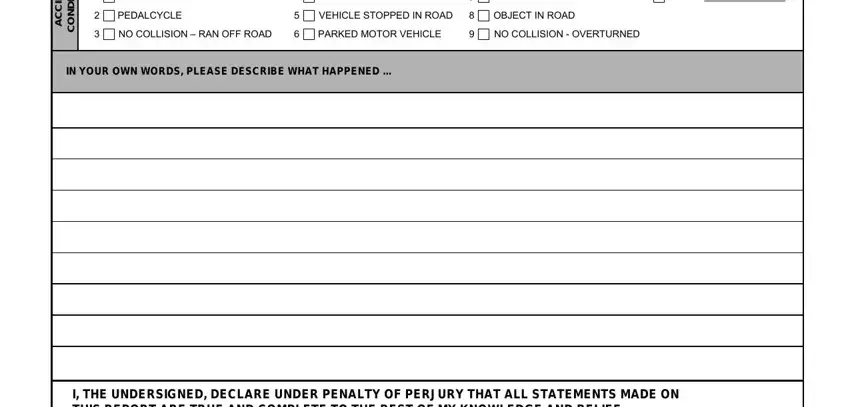
Provide a narrative description of how the accident occurred in your own words. Focus on the sequence of events, specifying actions taken by each driver and the conditions leading up to the accident.
5. Report Insurance Information
Fill in the insurance details for all vehicles involved. Include the insurance company name, policy number, and the policyholder's name and address.
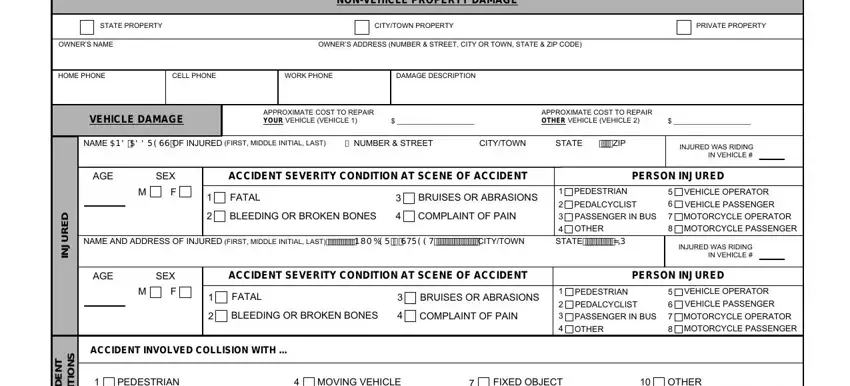
6. Note Injuries and Damages
Document any injuries or damages that occurred as a result of the accident. Include the names and addresses of those injured, describe the severity of the injuries, and estimate the cost of vehicle repairs.
7. Detail Non-Vehicle Property Damage
If the accident involved damage to property other than vehicles, such as a mailbox or fence, provide a detailed description of the property damaged, the owner’s name, and the estimated repair costs.
8. Complete Insurance Declaration
If applicable, fill in the section concerning uninsured or underinsured motorists.
9. Sign and Date the Report
Finalize the report by signing and dating it. Mail the completed form to the specified address for the Rhode Island Division of Motor Vehicles Accident Office.
