
Once you open the online PDF tool by FormsPal, you're able to fill in or modify osha gov 300a right here. We at FormsPal are committed to making sure you have the perfect experience with our editor by constantly adding new functions and enhancements. With all of these updates, using our tool gets better than ever! For anyone who is seeking to begin, here is what it will take:
Step 1: Hit the "Get Form" button above. It is going to open our editor so you could start filling in your form.
Step 2: With the help of our advanced PDF tool, you may accomplish more than merely fill in blanks. Edit away and make your docs look sublime with custom text added, or optimize the original input to excellence - all that comes with the capability to add any pictures and sign the document off.
It is actually straightforward to fill out the pdf with our practical tutorial! This is what you want to do:
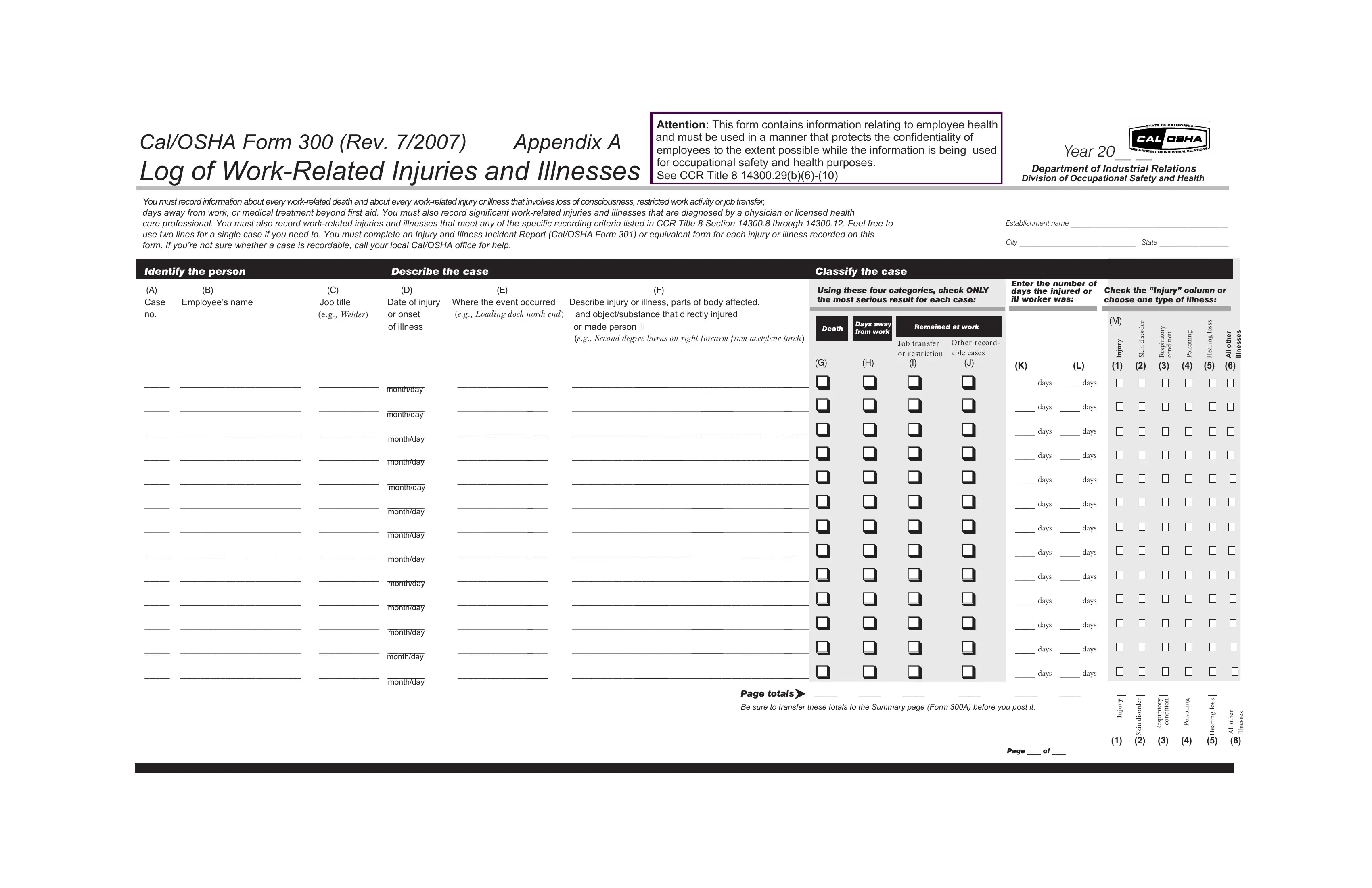
1. The osha gov 300a necessitates particular information to be entered. Make sure the next blanks are completed:
2. Once this section is finished, you'll want to put in the necessary specifics in monthday, monthday, monthday, monthday, monthday, monthday, monthday, monthday, monthday, monthday, monthday, monthday, days, days, and days allowing you to go to the next step.
Always be really attentive while filling in monthday and monthday, since this is where most people make mistakes.
3. This part is generally simple - complete every one of the empty fields in r e d r o s i d n i k S, y r o t a r i p s e R, Page of, s s o l g n i r a e H, and s e s s e n l l I in order to complete this process.

Step 3: When you have looked over the details in the document, simply click "Done" to finalize your FormsPal process. Create a 7-day free trial option at FormsPal and get instant access to osha gov 300a - readily available from your personal account. When you work with FormsPal, you can easily complete forms without having to get worried about personal information breaches or data entries being shared. Our protected software makes sure that your private information is maintained safe.