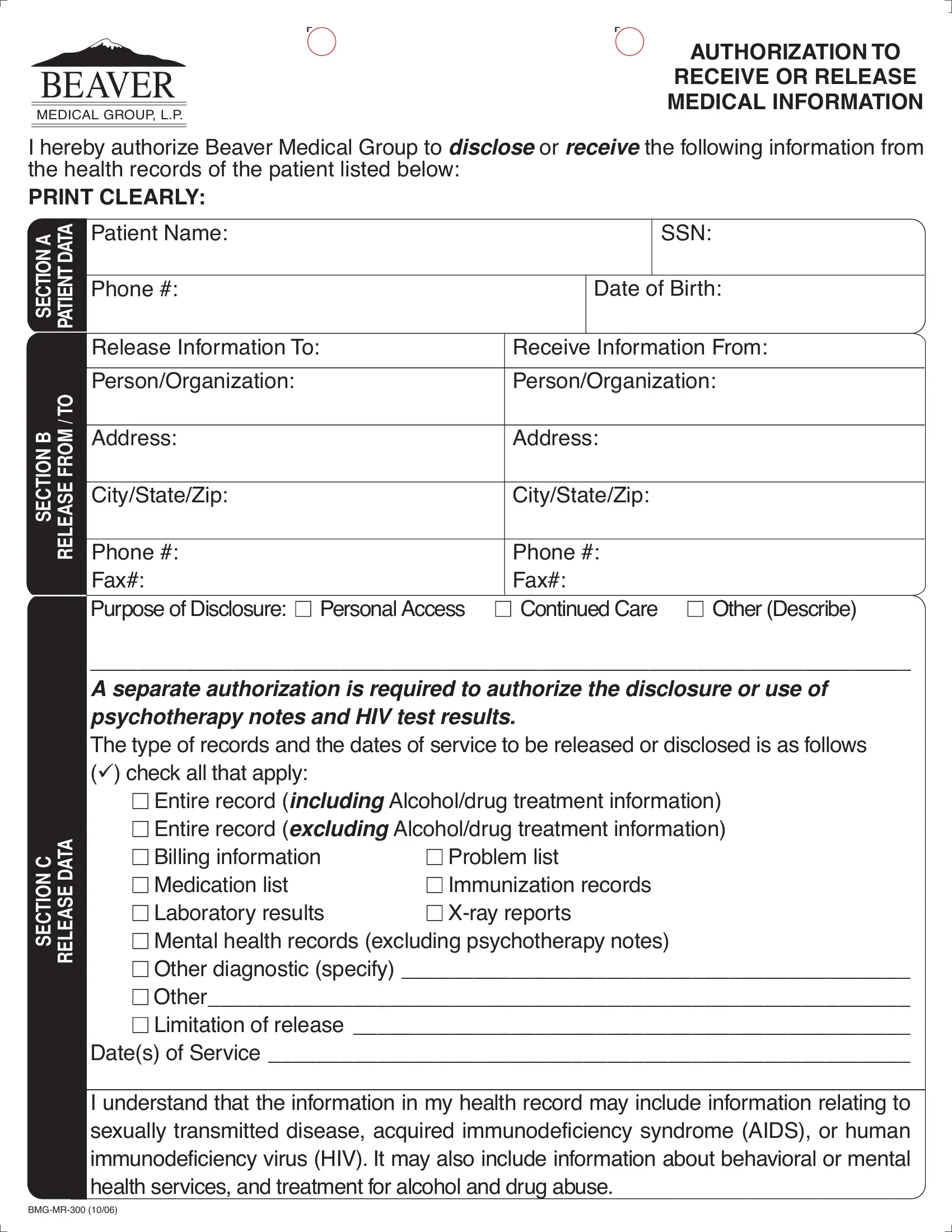
The Beaver Medical Group MR 300 form is a structured patient authorization for releasing health records. Beaver Medical Group, L.P., issues this document to patients who need to share specific medical information with authorized parties, such as other physicians, insurance companies, or government agencies.
The form is organized into clear sections. The patient identification section collects your name, date of birth, and contact details. A separate section identifies who is authorized to receive or release your records. Another section specifies the exact records covered by the authorization, including the type of information, the time period, and the purpose of the disclosure.
The MR 300 form provides special protections for sensitive health records under California law. Records related to HIV or AIDS status, mental health treatment, substance abuse treatment, and sexually transmitted diseases require explicit authorization. Even when you authorize the release of general health records, these sensitive categories must be separately consented to on the form.
Authorization is voluntary. Patients may revoke their consent at any time before Beaver Medical Group acts on the authorization by submitting a written revocation request. The authorization expires on the date you specify or when the stated purpose of the disclosure is complete, whichever comes first. Information already disclosed before revocation cannot be retracted.
| Question | Answer |
|---|---|
| Form Name | Beaver Bmg Mr 300 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | beaver medical records, BMG-MR-300, SSN, CFR |