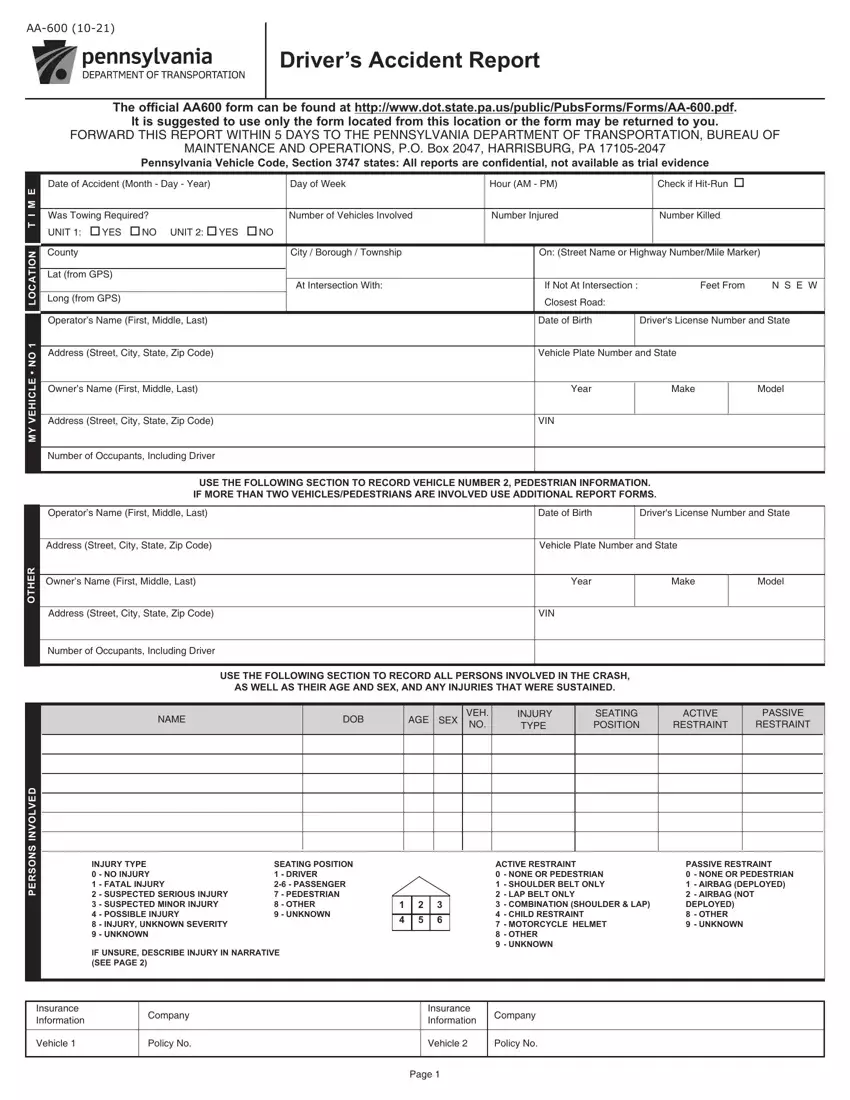
The AA-600 form is required for reporting motor vehicle accidents in Pennsylvania. It is essential for drivers involved in accidents that result in injury, death, or significant vehicle damage. Completing this form correctly ensures compliance with state laws.
1. Provide Accident Details
Enter the date, time, and accident location on the form. Be precise with the location, noting the county, city, or township, street name or highway number, and mile marker if applicable.
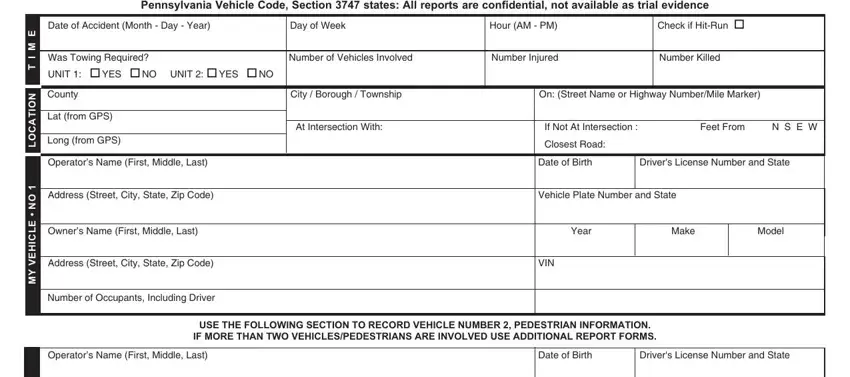
2. Document Vehicle and Driver Information
For each vehicle involved, fill in the operator’s name, address, date of birth, driver's license number, vehicle plate number, vehicle make and model, and the VIN. This information should be copied directly from the official driver’s license and vehicle registration card.
3. Describe the Accident
Provide a detailed description of the accident, including what happened before, during, and after the collision. Use the vehicle numbers designated on the form to reference each vehicle involved.

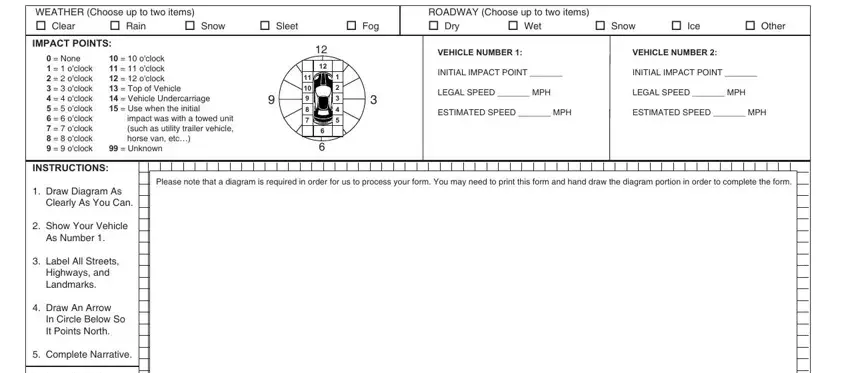
4. Complete the Diagram
Draw a diagram of the accident scene on the provided space in the form. Clearly show the movement of the vehicles, including all relevant streets, highways, landmarks, and an arrow indicating north.
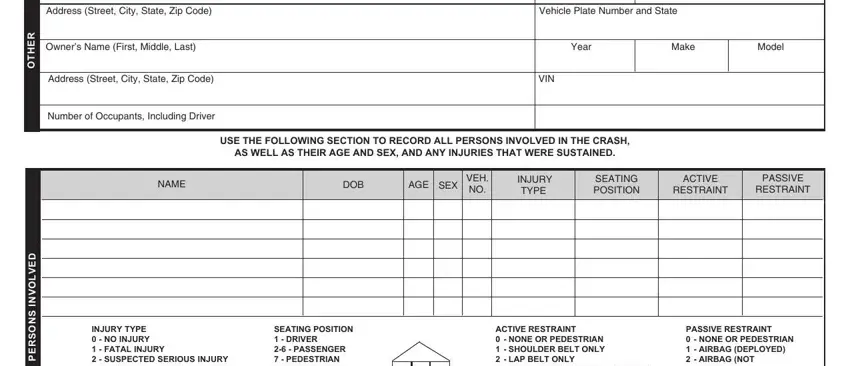
5. Report Injuries and Damage
Record the type of injuries sustained by all persons involved using the codes provided on the form for injury severity. Also, detail the damage area of each vehicle involved using the clock point system shown on the form.
6. Include Safety Restraint Information
Indicate the type of safety restraints used by each occupant during the accident, selecting the appropriate codes for active and passive restraints.
7. Confirm Additional Details
Verify if towing was required, the number of vehicles involved, and the number of occupants in each vehicle. If applicable, also indicate whether the police investigated the accident.
