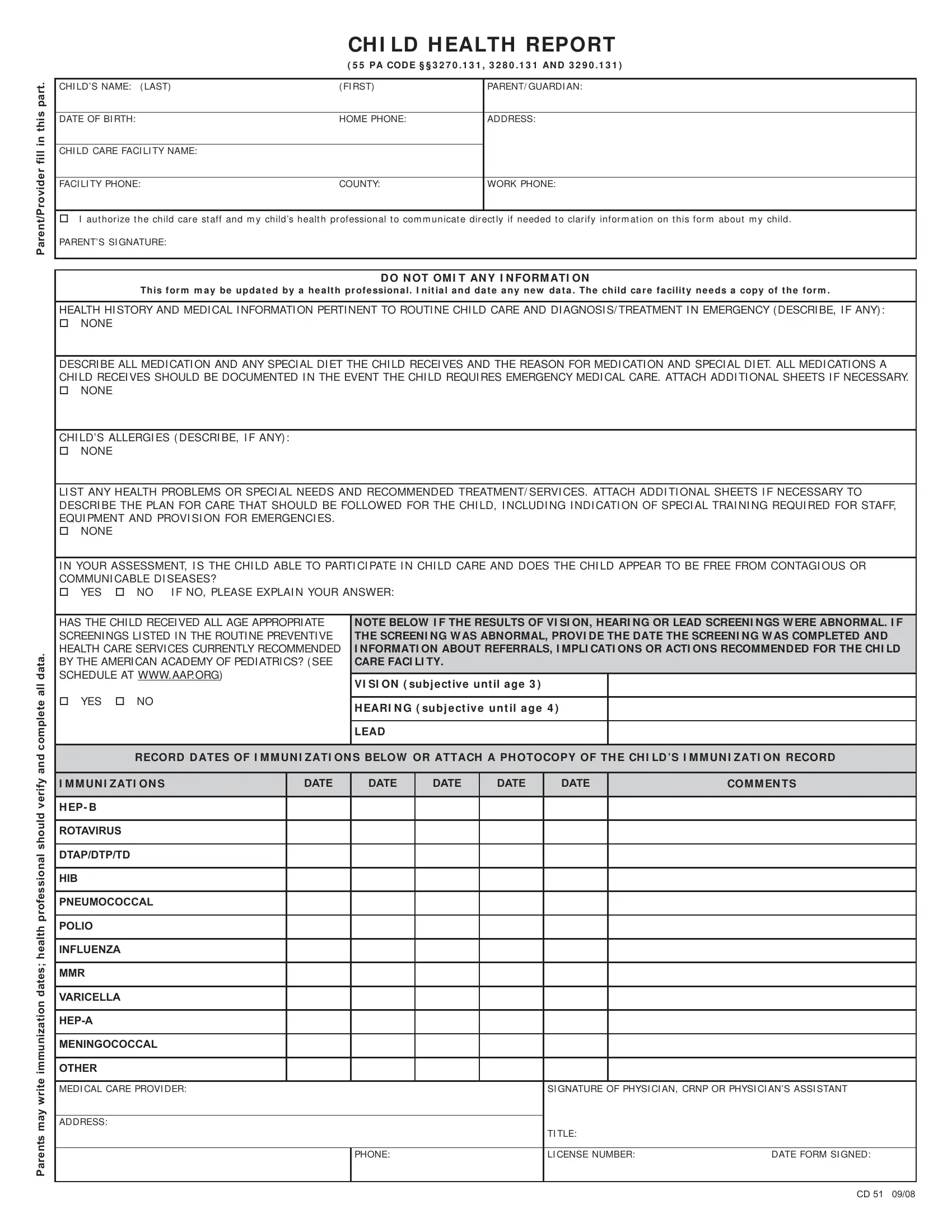
In the realm of child care and early education within Pennsylvania, ensuring the health and welfare of children is a priority that manifests in various state-mandated forms and procedures, among which the Pennsylvania Child Health Report Form stands out. Crafted to serve as a comprehensive record, this document is designed for completion by both the child's parent or guardian and the health care provider. It encompasses critical sections, including the child's personal information, health history, medicinal details, dietary needs if any, allergies, and specifics on any special needs or health problems that might impact their care or necessitate emergency interventions. Moreover, it inquires about the child's vaccination status in alignment with the American Academy of Pediatrics recommendations and screens for potential vision, hearing, or lead exposure issues, ensuring that child care providers are fully informed about the health status of the children under their care. This form not only facilitates communication between parents, health professionals, and child care staff but also requires that updates and new data are duly noted, ensuring the child receives appropriate care while attending the facility. By furnishing detailed health information and specifying any special requirements, this form plays a crucial role in safeguarding children's health and well-being in child care settings across Pennsylvania.
| Question | Answer |
|---|---|
| Form Name | Pa Child Report Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | pa form child health, child health report form, form child health report, pa child health report |
Parent/Provider fill in this part.
|
CH I LD H EALTH REPORT |
|
|
( 5 5 PA COD E § § 3 2 7 0 . 1 3 1 , 3 2 8 0 . 1 3 1 AN D 3 2 9 0 . 1 3 1 ) |
|
|
|
|
CHI LD’S NAME: ( LAST) |
( FI RST) |
PARENT/ GUARDI AN: |
|
|
|
DATE OF BI RTH: |
HOME PHONE: |
ADDRESS: |
|
|
|
CHI LD CARE FACI LI TY NAME: |
|
|
|
|
|
FACI LI TY PHONE: |
COUNTY: |
WORK PHONE: |
|
|
|
ニ#I aut hor ize t he child car e st aff and m y child’s healt h pr ofessional t o com m unicat e dir ect ly if needed t o clar ify infor m at ion on t his for m about m y child.
PARENT’S SI GNATURE:
D O N OT OM I T AN Y I N FORM ATI ON
Th is for m m a y be u pda t e d by a h e a lt h pr ofe ssion a l. I n it ia l a n d da t e a n y n e w da t a . Th e ch ild ca r e fa cilit y n e e ds a copy of t h e for m .
HEALTH HI STORY AND MEDI CAL I NFORMATI ON PERTI NENT TO ROUTI NE CHI LD CARE AND DI AGNOSI S/ TREATMENT I N EMERGENCY ( DESCRI BE, I F ANY) : ニ#NONE
DESCRI BE ALL MEDI CATI ON AND ANY SPECI AL DI ET THE CHI LD RECEI VES AND THE REASON FOR MEDI CATI ON AND SPECI AL DI ET. ALL MEDI CATI ONS A CHI LD RECEI VES SHOULD BE DOCUMENTED I N THE EVENT THE CHI LD REQUI RES EMERGENCY MEDI CAL CARE. ATTACH ADDI TI ONAL SHEETS I F NECESSARY. ニ#NONE
CHI LD’S ALLERGI ES ( DESCRI BE, I F ANY) : ニ#NONE
LI ST ANY HEALTH PROBLEMS OR SPECI AL NEEDS AND RECOMMENDED TREATMENT/ SERVI CES. ATTACH ADDI TI ONAL SHEETS I F NECESSARY TO DESCRI BE THE PLAN FOR CARE THAT SHOULD BE FOLLOWED FOR THE CHI LD, I NCLUDI NG I NDI CATI ON OF SPECI AL TRAI NI NG REQUI RED FOR STAFF, EQUI PMENT AND PROVI SI ON FOR EMERGENCI ES.
ニ#NONE
I N YOUR ASSESSMENT, I S THE CHI LD ABLE TO PARTI CI PATE I N CHI LD CARE AND DOES THE CHI LD APPEAR TO BE FREE FROM CONTAGI OUS OR COMMUNI CABLE DI SEASES?
ニ#YES |
ニ#NO I F NO, PLEASE EXPLAI N YOUR ANSWER: |
complete all data.
HAS THE CHI LD RECEI VED ALL AGE APPROPRI ATE SCREENI NGS LI STED I N THE ROUTI NE PREVENTI VE HEALTH CARE SERVI CES CURRENTLY RECOMMENDED BY THE AMERI CAN ACADEMY OF PEDI ATRI CS? ( SEE SCHEDULE AT WWW.AAP.ORG)
ニ#YES ニ#NO
NOTE BELOW I F THE RESULTS OF VI SI ON, HEARI NG OR LEAD SCREENI NGS W ERE ABNORMAL. I F THE SCREENI NG W AS ABNORMAL, PROVI DE THE DATE THE SCREENI NG W AS COMPLETED AND
I NFORMATI ON ABOUT REFERRALS, I MPLI CATI ONS OR ACTI ONS RECOMMENDED FOR THE CHI LD CARE FACI LI TY.
VI SI ON ( subj ect ive unt il age 3 )
H EARI N G ( su bj e ct iv e u n t il a ge 4 )
LEAD
Parents may write immunization dates; health professional should verify and
RECORD D ATES OF I M M UN I ZATI ON S BELOW OR ATTACH A PH OTOCOPY OF TH E CH I LD ’S I M M UN I ZATI ON RECORD
I M M UN I ZATI ON S |
DATE |
DATE |
DATE |
DATE |
DATE |
|
COM M EN TS |
|
|
|
|
|
|
|
|
H EP- B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ROTAVIRUS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DTAP/DTP/TD |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
HIB |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PNEUMOCOCCAL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
POLIO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INFLUENZA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MMR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
VARICELLA |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MENINGOCOCCAL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OTHER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDI CAL CARE PROVI DER: |
|
|
|
|
SI GNATURE OF PHYSI CI AN, CRNP OR PHYSI CI AN’S ASSI STANT |
||
|
|
|
|
|
|
|
|
ADDRESS: |
|
|
|
|
|
|
|
|
|
|
|
|
TI TLE: |
|
|
|
|
|
|
|
|
|
|
|
|
PHONE: |
|
|
LI CENSE NUMBER: |
DATE FORM SI GNED: |
|
|
|
|
|
|
|
|
|
CD 51 09/08