
The Confidential Morbidity Report form (CDPH 110C) can be filled out online with ease using FormsPal's PDF editor. Whether you are a physician, neurologist, or other healthcare professional with a mandatory communicable disease reporting obligation, our tool helps you complete the process quickly and accurately. We continually update our editor based on user feedback from healthcare providers and medical professionals.
When to Use the Confidential Morbidity Report
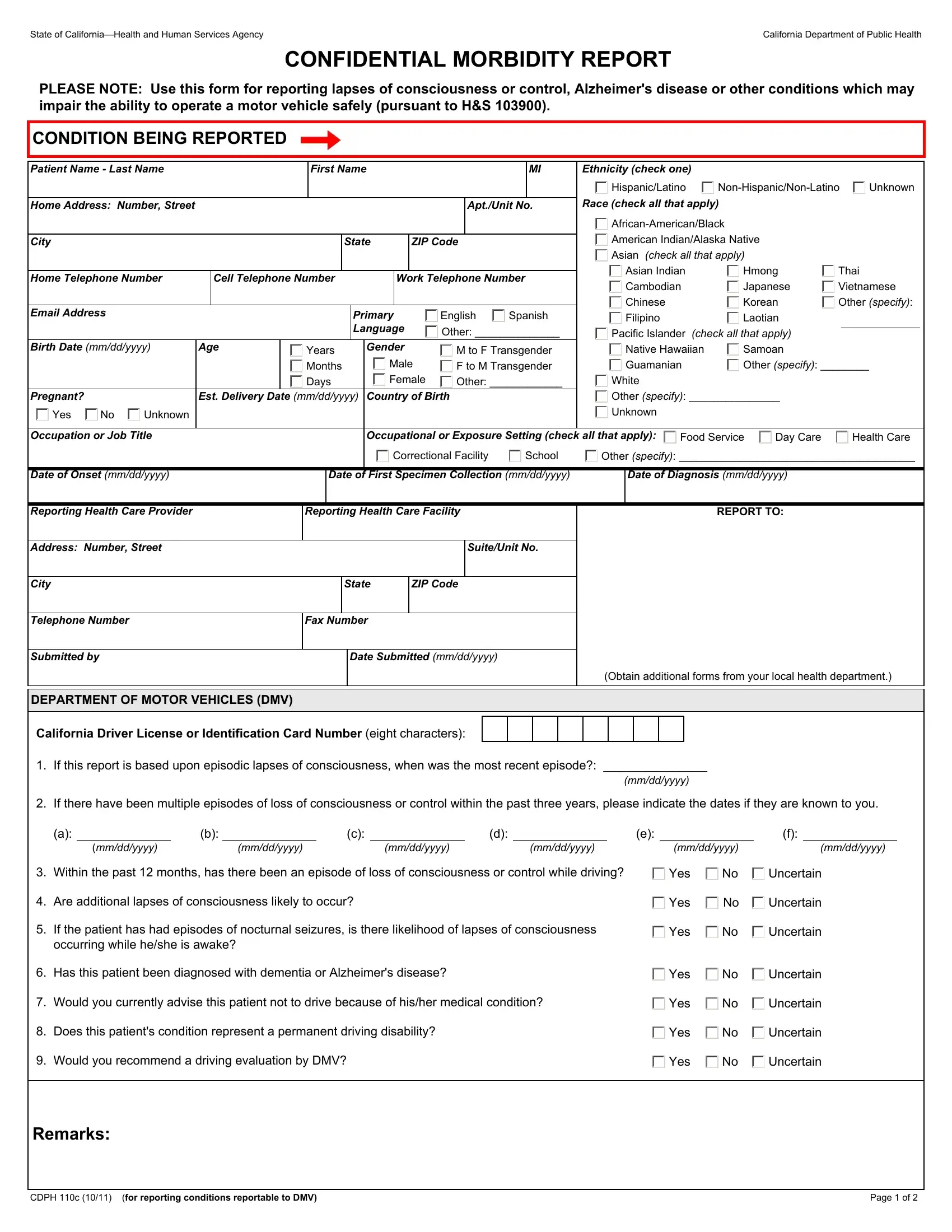
Submit this report when a patient has a health condition that may impair their ability to drive safely. Reportable conditions include lapses of consciousness, Alzheimer's disease, uncontrolled seizures, and other neurological or cardiovascular conditions. Under California Health and Safety Code Section 103900, the reporting process is a legal obligation for licensed healthcare providers. After completing the form, submit it to the local county public health officer. Contact your county health department for specific fax numbers, mailing addresses, and program resources. The county public health officer will review the case and may refer it to the California DMV for further testing or license evaluation services.
Steps to Complete the CDPH 110C Form
Step 1: Click the orange "Get Form" button above. This will open our PDF tool so you can begin filling out your form.
Step 2: After you start the PDF editor, you will notice the document ready to be filled out. You can fill in various fields, add text, edit the original content, insert illustrations or photos, sign the document, and more.
This document requires particular information to be entered. Take the time to fill in precisely what is expected:
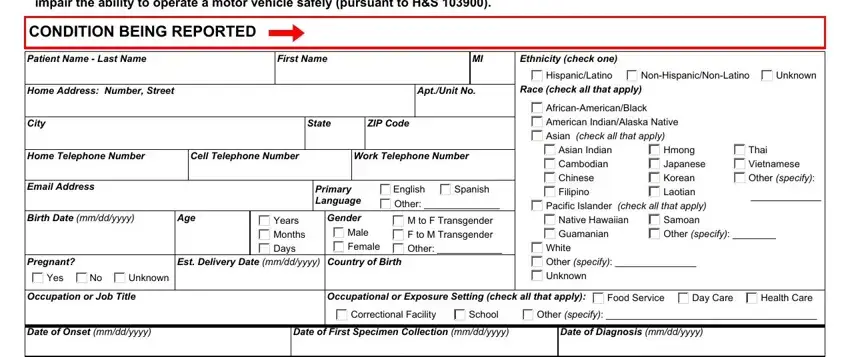
1. When filling in the morbidity report, start with the section containing these fields:
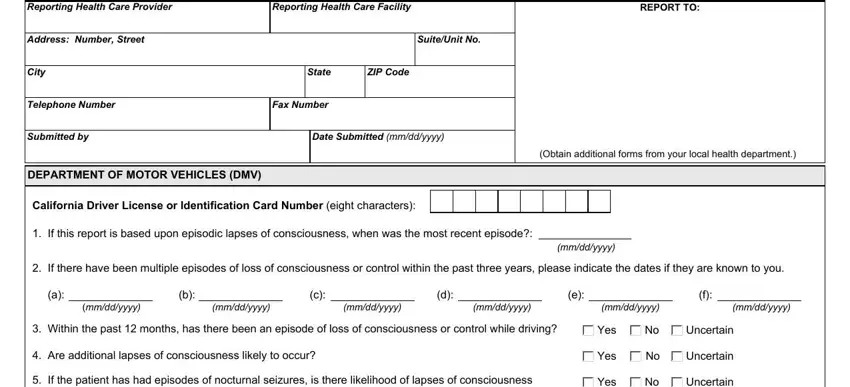
2. Next, fill out all of these fields - Reporting Health Care Provider, Reporting Health Care Facility, REPORT TO, Address Number Street, Suite No, Unit No, City, State, ZIP Code, Telephone Number, Fax Number, Submitted by, Date Submitted mm/dd/yyyy, DEPARTMENT OF MOTOR VEHICLES DMV, California Driver License or ID, and contact information for obtaining additional forms. Make sure to double check that everything has been entered correctly before continuing.
3. The following section covers: whether the patient has had episodes of consciousness loss, whether the patient has been diagnosed with a reportable condition, your current clinical recommendation regarding driving, whether the patient's condition affects their safety on the road, whether you would recommend a driving evaluation, and remarks for the county public health officer. Complete the CDPH case section for reporting conditions.
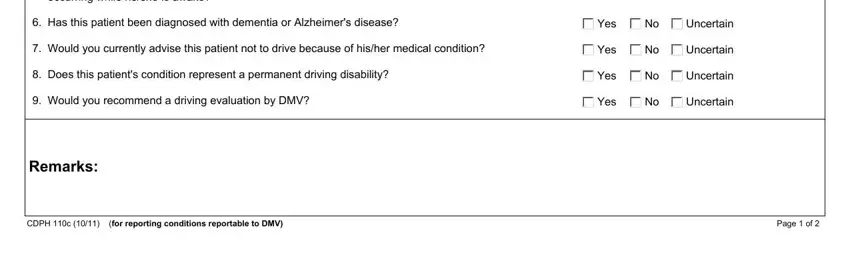
4. The final section covers CDPH case number and page reference fields, which are essential for completing and submitting the report to the county public health department.
Healthcare providers frequently make errors in the CDPH case section. Review your entries carefully before submitting to the public health officer.
Step 3: Confirm that the information is accurate and click "Done" to proceed. After registering a free trial account, you will be able to download the completed morbidity report or send it by email. The form will also be available in your personal account page with your changes. FormsPal is committed to protecting the privacy of all users and keeping personal data secure in our editor.
Related California Health and DMV Forms
If you work with California health reporting and motor vehicle documents, these related forms may also be useful for your practice or public health program:
- Confidential STD Morbidity Report Form - for reporting sexually transmitted diseases to county public health authorities
- California DMV DL 546 Form - Verification of Residency used in DMV licensing processes
- California Advance Healthcare Directive Form - for patients to document healthcare decision preferences
- CA DMV DL 546A Form - supplemental California DMV document for driver licensing services