
How to Fill Out the CA DMV DL 546A Form Online
Filling out the California DMV DL 546A Physician's Health Report online is straightforward with our PDF tool. You can complete the health questionnaire, review each section with your physician, and save or print the finished form. Follow the steps below to get started.
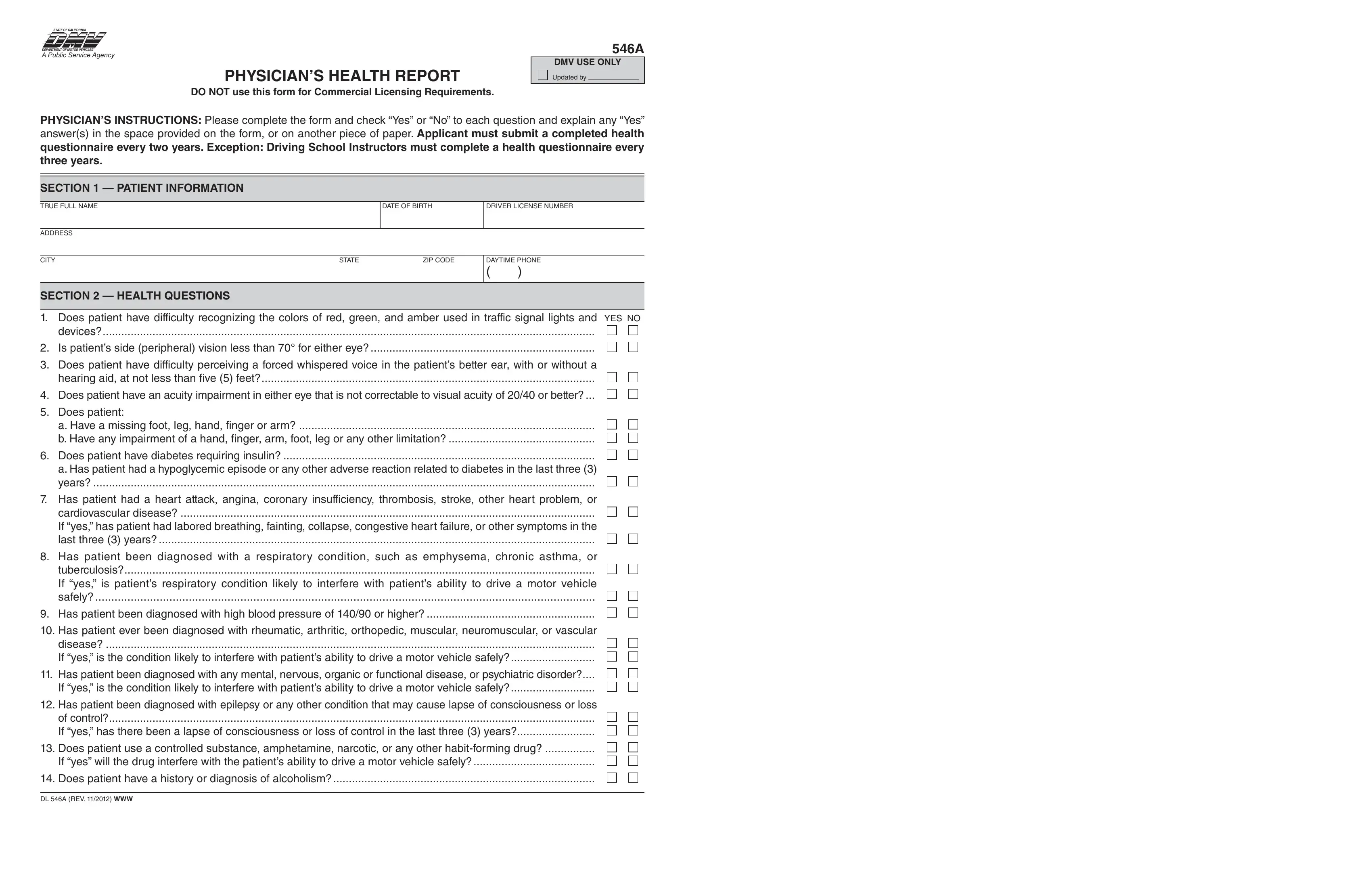
Step 1: Press the "Get Form" button at the top of this page to open our PDF editor. All editable fields in the DL 546A form will be available immediately.
Step 2: Complete the patient information and physician assessment sections. The form requires details about heart conditions, neurological history, vision, hearing, blood pressure readings, and any controlled substance use. Make sure your physician reviews the fields for: has patient had a heart attack, has patient been diagnosed with a cardiovascular condition, neurological disorders, vision correction notes, and the physician's name and office address.
Step 3: Complete the remaining fields including uncorrected and corrected vision measurements (UNCORRECTED and CORRECTED both left and right), blood pressure readings (systolic and diastolic), whether contact lenses are well adapted, and whether the applicant is applying as a House Car driver. The physician signs the form and prints their name, license number, and office address. The applicant also signs under penalty of perjury.
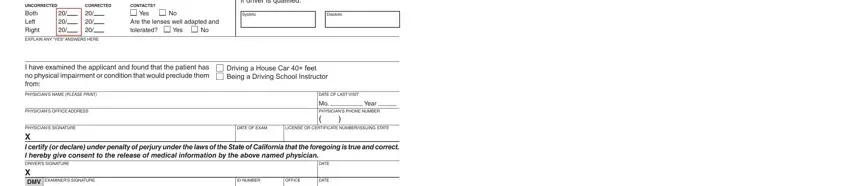
Be careful when entering blood pressure readings and vision correction values, as errors in these fields are the most common reason the DMV requests a revised submission.
Step 4: Review all fields for accuracy. When you are satisfied, click "Done" to save the completed DL 546A form. Download the PDF and share it with your physician for review and signature before mailing to the California DMV Medical Unit.
Tips for Completing the DL 546A Health Questionnaire
Bring a copy of your current prescription list and any recent lab results to your physician appointment before completing form DL 546A. The DMV evaluates several chronic conditions that require supporting documentation, including diabetes A1C records and cardiology reports. Using clear, legible handwriting or the online editor reduces processing delays.
Related California DMV Forms
If you need other California DMV documents, FormsPal offers additional forms to help you manage your licensing requirements:
- California DMV DL 546 Form - the standard version of the Physician's Health Report without the "A" suffix
- CA DMV Form 488C - used for occupational licensing applications
- CA DMV Form DL 44 - driver's license application form
- CA DMV 10-Year Driving Record - request your full driving history
FormsPal makes it easy to fill out, save, and download any of these California DMV pdf forms from any device. All form data you enter is kept private and is not shared with third parties.