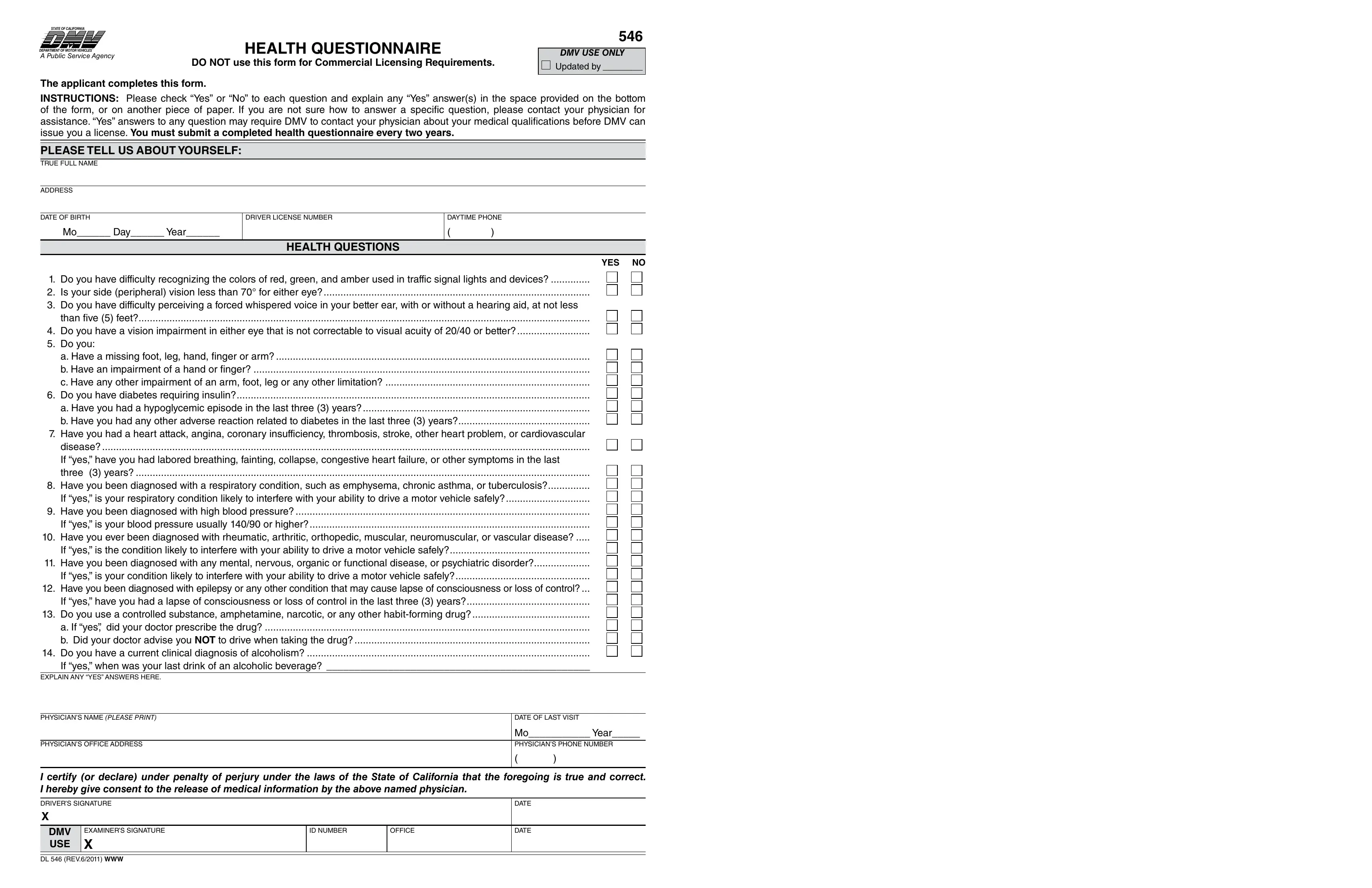
The California DMV DL 546 form, formally called the Health Questionnaire, is required for residents who apply for a new driver's license or are selected for a medical fitness review by the California Department of Motor Vehicles. It helps the DMV confirm that an applicant's health status does not pose a safety risk on public roads.
Any California resident applying for a new driver's license must complete the DL 546. The DMV also requests the form during license renewals when a health concern has been flagged, or when a physician, law enforcement officer, or other licensed professional has filed a report about a driver's medical fitness. Drivers over a certain age may receive a mandatory request to complete the form as part of a routine review cycle.
The DL 546 asks about a range of conditions that could affect driving ability. Applicants must disclose vision problems such as reduced field of view or night blindness, hearing loss, heart conditions including irregular heartbeat or recent cardiac events, seizure disorders, diabetes requiring insulin treatment, and conditions that affect the use of hands, feet, or limbs. Mental health conditions and any recent hospitalizations that limit physical function are also included.
If you answer yes to any item on the DL 546, the DMV opens a medical review for your case. Depending on the condition disclosed, you may be asked to submit a completed CA DMV DL 546A physician form signed by your doctor. The review typically takes 2 to 4 weeks. You may continue driving during this period unless the DMV sends written notice to the contrary. Once the review concludes, the DMV will notify you by mail of their decision.
First-time applicants for a California driver's license also need to file the California DMV DL 44 application form along with the DL 546. Applicants for a commercial driver's license may additionally need the DL 546A, which includes a section for the examining physician to complete. For a general-purpose health disclosure template, see the health questionnaire form at FormsPal.
| Question | Answer |
|---|---|
| Form Name | California DMV DL 546 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | dmv 546 health questionnaire, dmv medical questionnaire, ca dmv health questionnaire fillable 546, dmv health questionnaire, california dmv health questionnaire |