
Our PDF editor you are going to work with was developed by our best programmers. It is possible to get the pennsylvania form payroll document fast and effortlessly with this software. Just keep up with this specific guideline to begin with.
Step 1: Select the button "Get Form Here" on the site and select it.
Step 2: Now you can enhance the pennsylvania form payroll. You can use our multifunctional toolbar to include, delete, and modify the content material of the file.
These particular segments will frame the PDF form that you will be filling out:
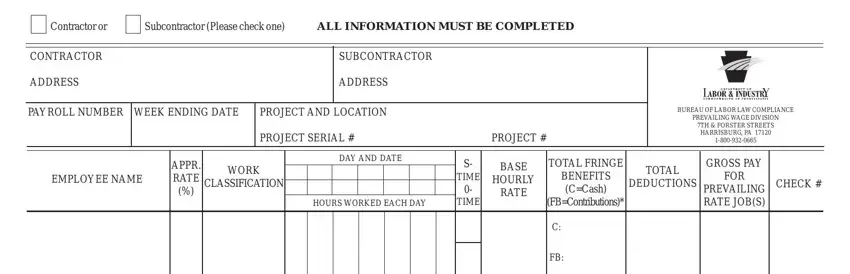
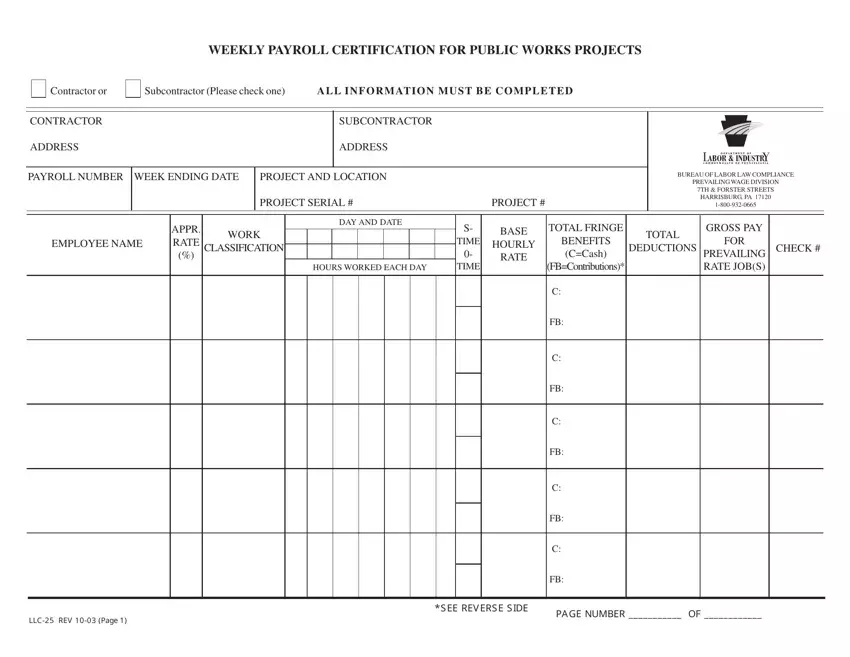
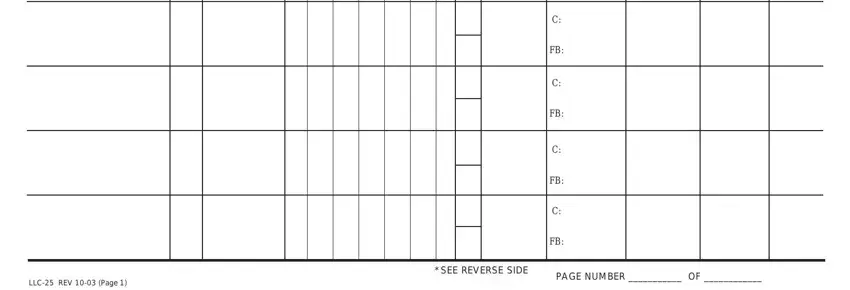
Write down the details in the LLC, REV, Page SEE, REVERSE, SIDE and PAGE, NUMBER, OF area.
In the segment discussing CERTIFIED, STATEMENT, OF, COMPLIANCE and The, undersigned, certifies, that make sure you put down some appropriate particulars.
The The, undersigned, certifies, that The, undersigned, is NAME, TITLE, ADDRESS, DATE, SIGNATURE, and TITLE box could be used to point out the rights and obligations of all sides.
Finalize by reviewing the next sections and filling out the relevant details: SEAL, LLC, REV, Page and of, AD

Step 3: Select the button "Done". Your PDF form is available to be transferred. You can download it to your pc or email it.
Step 4: To protect yourself from potential upcoming challenges, you should definitely obtain no less than a couple of duplicates of every form.
