
Any time you want to fill out personal care reportable incident form, you don't have to download any programs - just give a try to our online tool. To keep our tool on the cutting edge of efficiency, we work to implement user-oriented features and enhancements regularly. We are at all times thankful for any suggestions - join us in revolutionizing PDF editing. To begin your journey, take these simple steps:
Step 1: Press the "Get Form" button above on this webpage to open our PDF editor.
Step 2: Using this handy PDF editing tool, it's possible to accomplish more than simply fill in blank fields. Express yourself and make your docs seem professional with custom text added, or tweak the original input to perfection - all supported by an ability to incorporate any kind of photos and sign it off.
This form needs some specific details; to ensure accuracy and reliability, be sure to adhere to the recommendations further down:
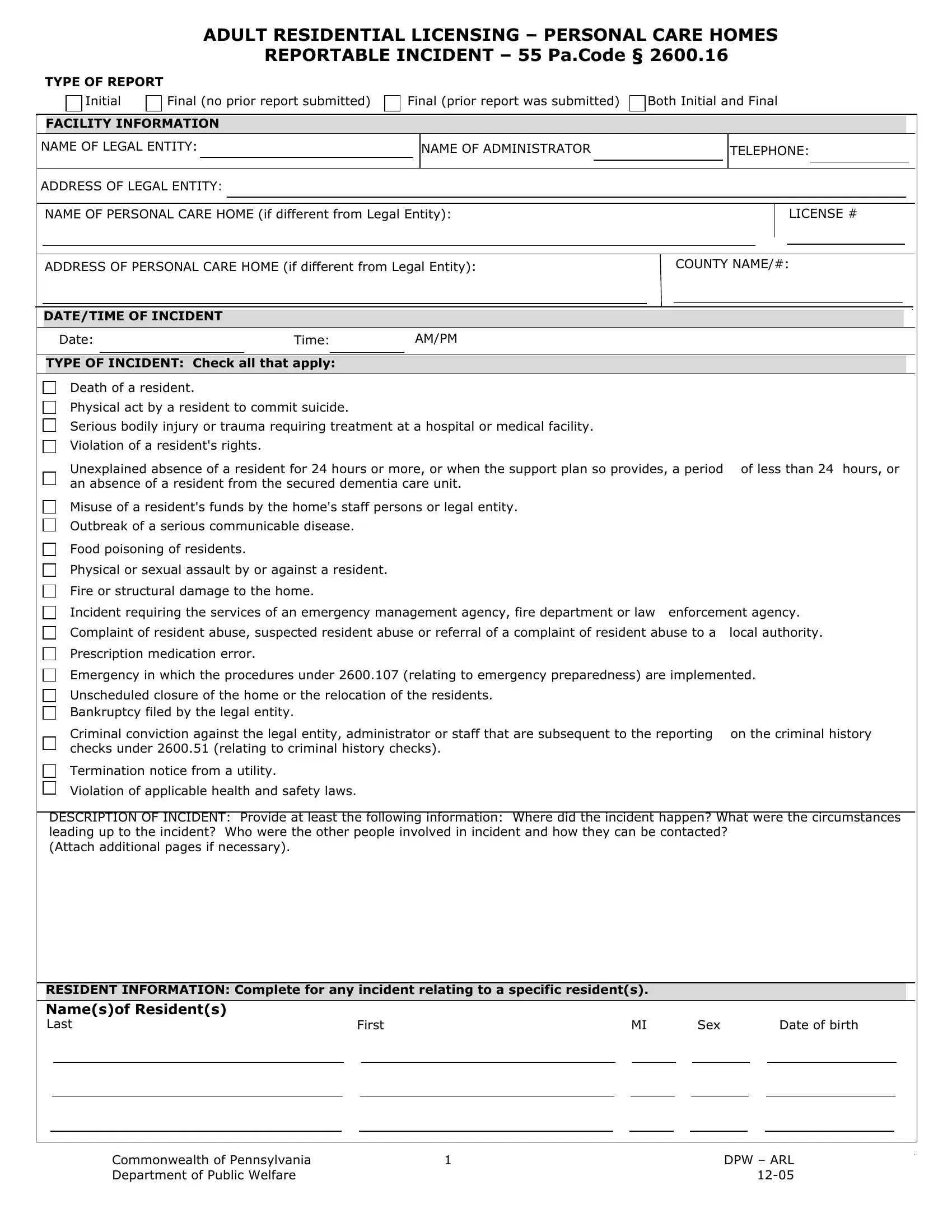
1. First, when filling in the personal care reportable incident form, beging with the section that has the following blanks:
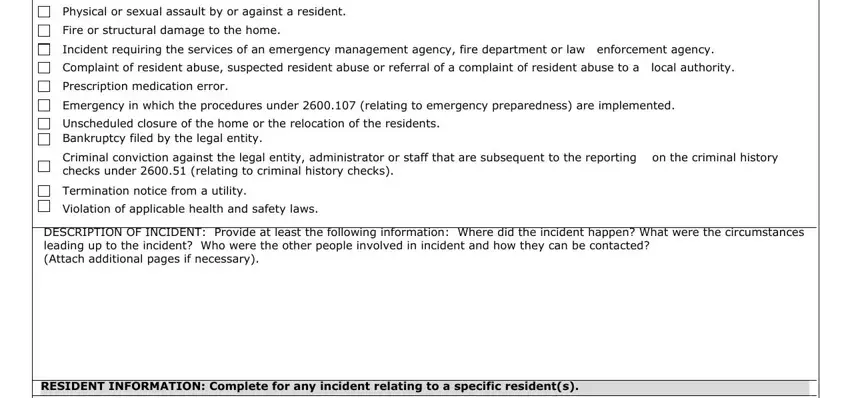
2. Once the previous segment is completed, you're ready insert the needed specifics in Physical or sexual assault by or, Fire or structural damage to the, Incident requiring the services of, Complaint of resident abuse, Prescription medication error, Emergency in which the procedures, Unscheduled closure of the home or, Criminal conviction against the, Termination notice from a utility, Violation of applicable health and, DESCRIPTION OF INCIDENT Provide at, and RESIDENT INFORMATION Complete for allowing you to go to the 3rd stage.
3. Completing Namesof Residents Last, First, Sex, Date of birth, Commonwealth of Pennsylvania, and DPW ARL is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
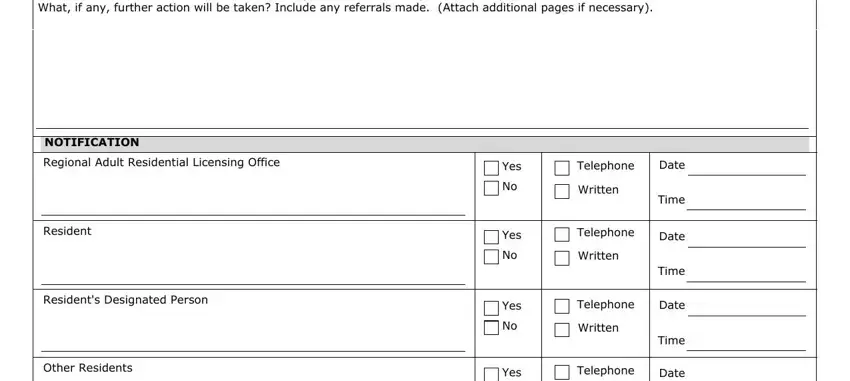
4. Completing FOLLOWUP ACTION TAKEN What action, NOTIFICATION, Regional Adult Residential, Resident, Residents Designated Person, Other Residents, Yes, Yes, Yes, Yes, Telephone, Date, Written, Telephone, and Written is essential in the fourth form section - don't forget to invest some time and take a close look at each and every empty field!
5. To conclude your form, this final segment has a couple of extra blanks. Typing in Others, Yes, Written, Time, Telephone, Date, Written, Time, CONTACT INFORMATION, Name of person completing report, Title, Datetime this report was completed, Date, Time, and AMPM should conclude everything and you can be done very fast!
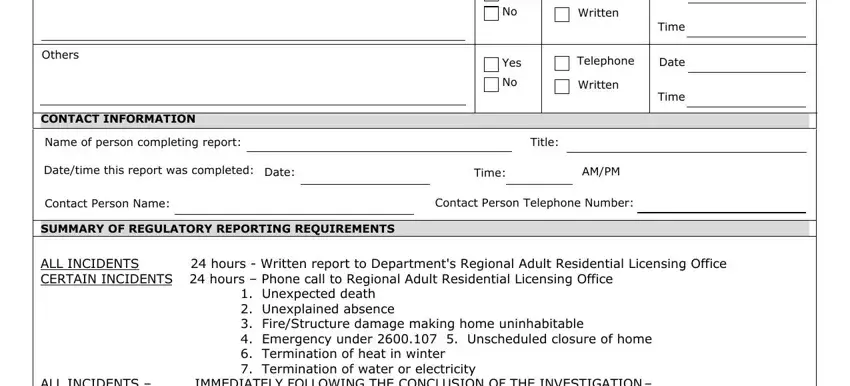
As to Date and Others, ensure that you don't make any mistakes in this current part. These are thought to be the key ones in this page.
Step 3: Prior to moving on, you should make sure that form fields are filled out properly. Once you are satisfied with it, click on “Done." Get hold of the personal care reportable incident form as soon as you join for a free trial. Instantly use the pdf file within your FormsPal account, along with any modifications and changes automatically synced! Whenever you work with FormsPal, you can complete forms without the need to worry about personal information breaches or records being shared. Our protected platform helps to ensure that your private details are kept safely.