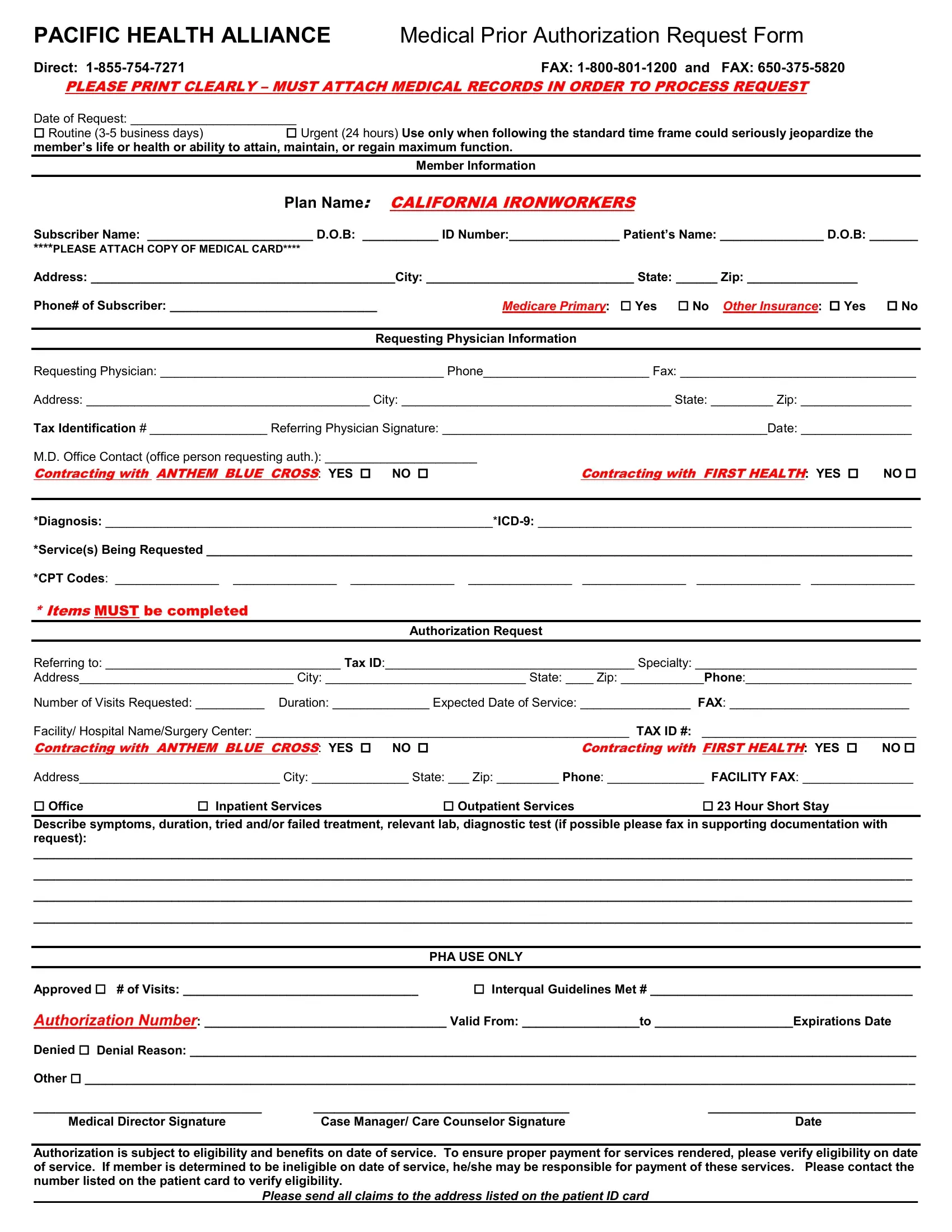
The Pacific Health Alliance Medical Prior Authorization Request Form embodies a critical process in healthcare management, serving as a gateway for securing necessary medical services. This detailed form, designed for streamlined communication between healthcare providers and the insurance company, necessitates comprehensive information to ensure a smooth authorization process. It outlines specific sections for both routine and urgent requests, clearly marking the urgency of medical intervention required and emphasizing the need for attached medical records to process the request efficiently. From capturing essential member and physician details, such as names, contact information, and insurance specifics, to listing the requested medical services with appropriate diagnostic codes, every section is tailored to gather requisite data. Moreover, the form goes beyond mere data collection by instructing providers on how to classify the requested services—ranging from office visits to inpatient or outpatient services—and demanding a detailed account of the patient's symptoms, treatment history, and diagnostic tests. The addition of sections indicating whether the provider is contracting with significant insurers like Anthem Blue Cross and First Health highlights the form's role in navigating the complex insurance landscape. Ultimately, this document culminates in a section for Pacific Health Alliance's use only, delineating the approval or denial of the request, thus governing the patient's access to the proposed healthcare services based on criteria like eligibility and benefit coverage on the service date, underscoring the importance of verification to avoid unexpected patient liabilities.
| Question | Answer |
|---|---|
| Form Name | Pacific Alliance Medical Group Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | community care alliance prior auth form for surger, pacific health alliance prior authorization, health alliance prior auth forms, central california alliance prior authorization form dme fillable |
