
When working in the online tool for PDF editing by FormsPal, you are able to complete or alter patient demographic form pdf here and now. The tool is consistently improved by us, acquiring new awesome functions and turning out to be better. Should you be looking to get going, here's what it takes:
Step 1: Access the PDF form in our editor by hitting the "Get Form Button" at the top of this page.
Step 2: As you access the online editor, there'll be the form prepared to be filled in. Other than filling in different blank fields, you may as well perform other sorts of actions with the PDF, namely putting on any words, editing the original textual content, adding images, affixing your signature to the document, and a lot more.
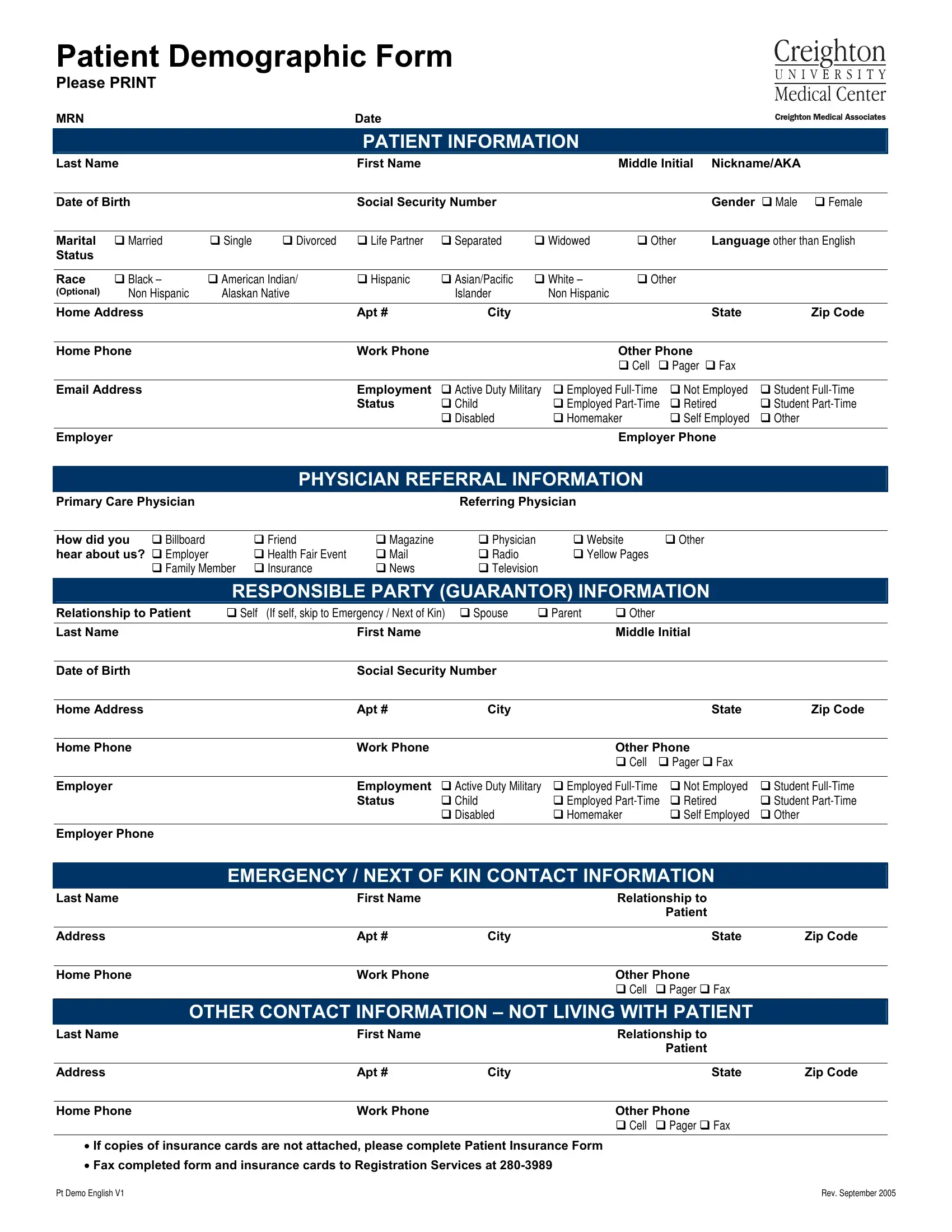
This document will need particular information to be filled out, therefore be sure to take whatever time to enter exactly what is required:
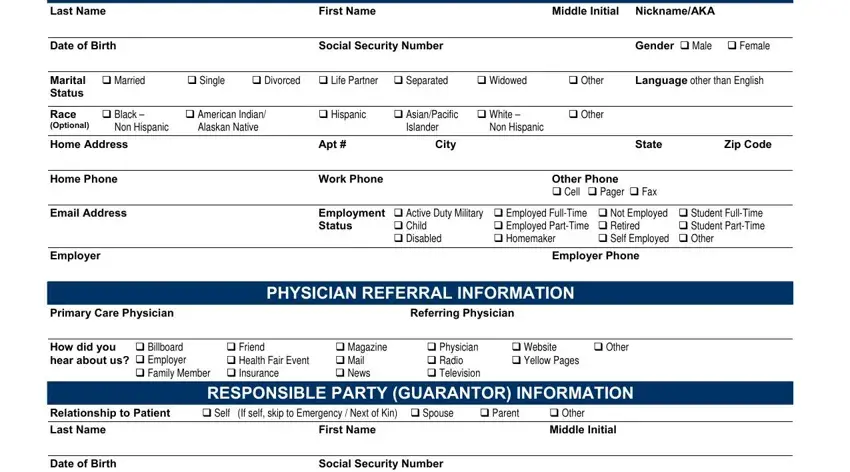
1. It is crucial to fill out the patient demographic form pdf accurately, thus take care when working with the areas including these fields:
2. The subsequent stage is usually to complete all of the following fields: Home Address, Apt, City, State, Zip Code, Home Phone, Employer, Work Phone, Other Phone cid Cell cid Pager cid, Employment Status, cid Active Duty Military cid Child, cid Employed FullTime cid Employed, cid Not Employed cid Retired cid, cid Student FullTime cid Student, and Employer Phone.
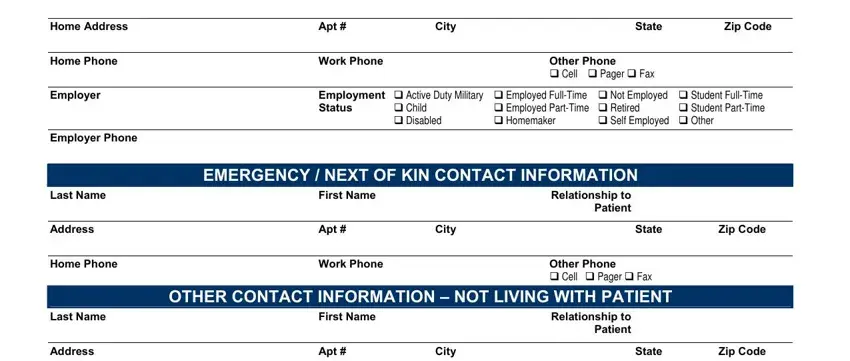
3. This 3rd section should be quite simple, Home Phone, Work Phone, Other Phone cid Cell cid Pager cid, If copies of insurance cards are, Pt Demo English V, and Rev September - all these form fields is required to be filled in here.

It's easy to make an error when completing your Rev September, for that reason you'll want to go through it again prior to when you submit it.
Step 3: Check everything you've entered into the blank fields and then click the "Done" button. Sign up with us right now and instantly gain access to patient demographic form pdf, prepared for download. Each and every modification you make is handily saved , so that you can modify the form at a later stage if required. FormsPal is focused on the confidentiality of all our users; we make sure that all personal information used in our tool is protected.