
With the help of the online PDF editor by FormsPal, it is easy to complete or alter ACCT here. The tool is constantly upgraded by our staff, getting new features and becoming better. Here's what you will have to do to get going:
Step 1: First of all, open the pdf tool by pressing the "Get Form Button" above on this site.
Step 2: This tool will allow you to customize your PDF in a variety of ways. Modify it by adding customized text, correct existing content, and include a signature - all within several clicks!
Completing this PDF typically requires thoroughness. Make sure every single blank field is filled in accurately.
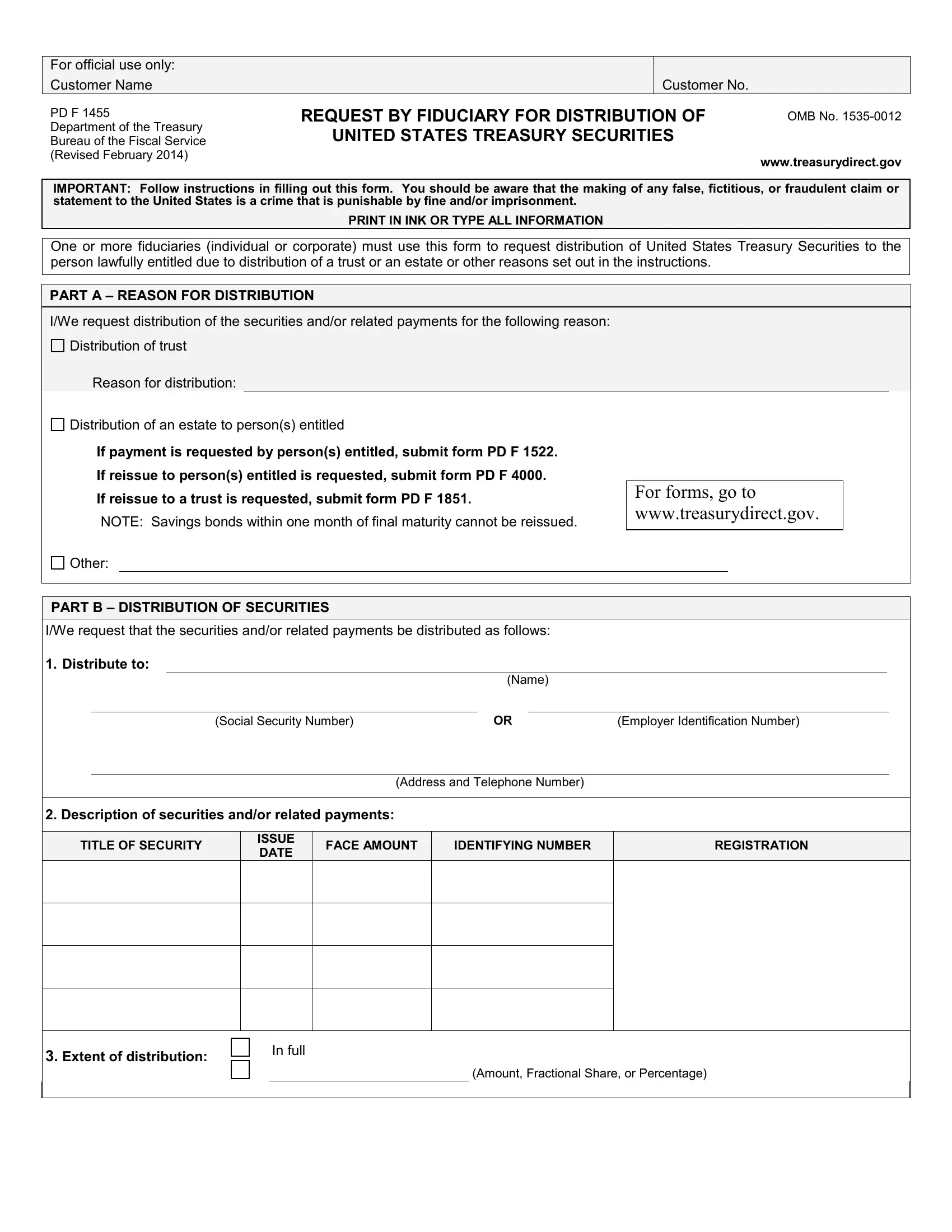
1. The ACCT needs certain details to be entered. Ensure that the following blank fields are complete:
2. Immediately after the prior array of blanks is completed, go on to type in the applicable information in all these: FACE AMOUNT, IDENTIFYING NUMBER, REGISTRATION, ISSUE DATE, TITLE OF SECURITY, Extent of distribution, In full, and Amount Fractional Share or.
3. The following segment is all about IWe request that the securities, Distribute to, Social Security Number, Name, Address and Telephone Number, Employer Identification Number, FACE AMOUNT, IDENTIFYING NUMBER, REGISTRATION, ISSUE DATE, Description of securities, TITLE OF SECURITY, Extent of distribution, In full, and Amount Fractional Share or - complete every one of these blank fields.
In terms of Name and FACE AMOUNT, ensure you get them right in this section. Both these could be the most important ones in this PDF.
4. The next section requires your details in the following parts: IWe request that the securities, Distribute to, Social Security Number, Employer Identification Number, Name, Address and Telephone Number, Description of securities, TITLE OF SECURITY, ISSUE DATE, FACE AMOUNT, IDENTIFYING NUMBER, REGISTRATION, Extent of distribution, In full, and Amount Fractional Share or. It is important to give all of the required information to go onward.
5. As you draw near to the finalization of the document, you will find a couple extra points to do. Mainly, You must wait until you are in the, Sign Here, Applicants Signature, Applicants Title, Number and Street Rural Route or, City, State, ZIP Code, Daytime Telephone Number, EMail Address, Instructions to Certifying Officer, I CERTIFY that, Name of Person Who Appeared, whose identity is known or, and proven to me personally appeared should be done.
Step 3: Be certain that the information is right and then just click "Done" to conclude the project. Get the ACCT the instant you subscribe to a 7-day free trial. Immediately use the document within your personal account page, together with any modifications and changes being automatically synced! FormsPal offers protected form completion devoid of personal data record-keeping or sharing. Rest assured that your information is in good hands with us!