
You could work with Pebb Form 107 026 effortlessly by using our PDFinity® online tool. To have our tool on the forefront of efficiency, we aim to put into action user-driven features and enhancements on a regular basis. We're routinely happy to get suggestions - assist us with reshaping PDF editing. Here's what you'd have to do to get started:
Step 1: Click on the "Get Form" button at the top of this page to open our PDF tool.
Step 2: When you open the tool, you will notice the form prepared to be filled out. Aside from filling out different blanks, it's also possible to perform several other things with the PDF, including writing any text, modifying the original textual content, adding graphics, putting your signature on the form, and more.
In order to finalize this document, make sure you provide the information you need in each area:
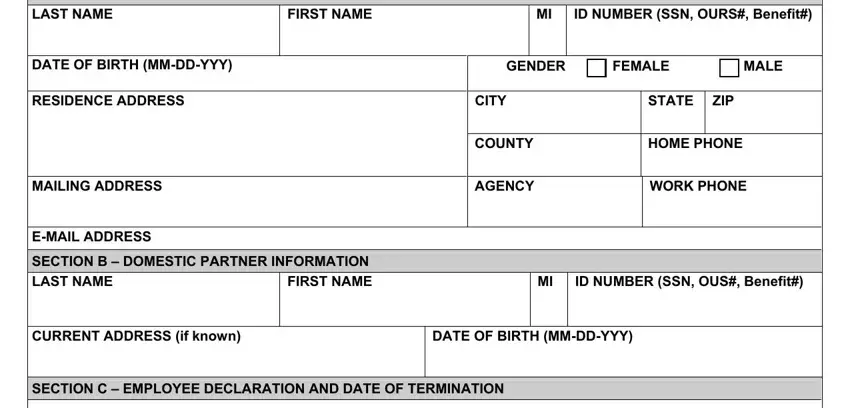
1. It is recommended to fill out the Pebb Form 107 026 correctly, thus be careful while working with the segments containing these specific blanks:
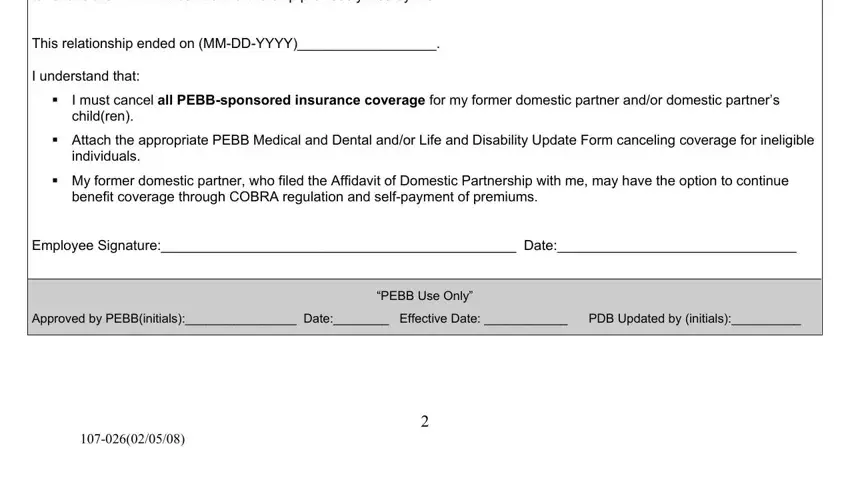
2. After performing the last step, go to the subsequent part and enter the essential particulars in all these blanks - to revoke the PEBB Affidavit of, This relationship ended on MMDDYYYY, I understand that, cid, I must cancel all PEBBsponsored, cid Attach the appropriate PEBB, individuals, cid My former domestic partner who, benefit coverage through COBRA, Employee Signature Date, Approved by PEBBinitials Date, and PEBB Use Only.
You can certainly make errors while filling out the cid, hence make sure to go through it again prior to deciding to finalize the form.
Step 3: Spell-check the information you have entered into the form fields and click on the "Done" button. Make a 7-day free trial account at FormsPal and obtain immediate access to Pebb Form 107 026 - with all transformations saved and available in your personal account page. We don't share or sell any details you use whenever completing documents at our website.